Surgical Trials

IPa-Gastric Trial
Magnus Nilsson


LOLIPOP trial: Long-term outcomes of lidocaine for post-operative chronic post-surgical pain
Chloe Beard, Leah Fleming, Annie Thomas, Rachel Brierley

Perf-Act BreCon: A Prospective Case-control Study to Compare Tissue Perf usion between RetrA ctors and Non-retractors during Immediate Bre ast ReCon struction
Amit Agrawal, Alex Azevado

Type B dissections: keeping it “uncomplicated” in a complicated world
Bianca Biersteker, Joost van der Vorst, Jacob Budtz-Lilly

Pain and reward in emergency surgery trials
Mark Edwards
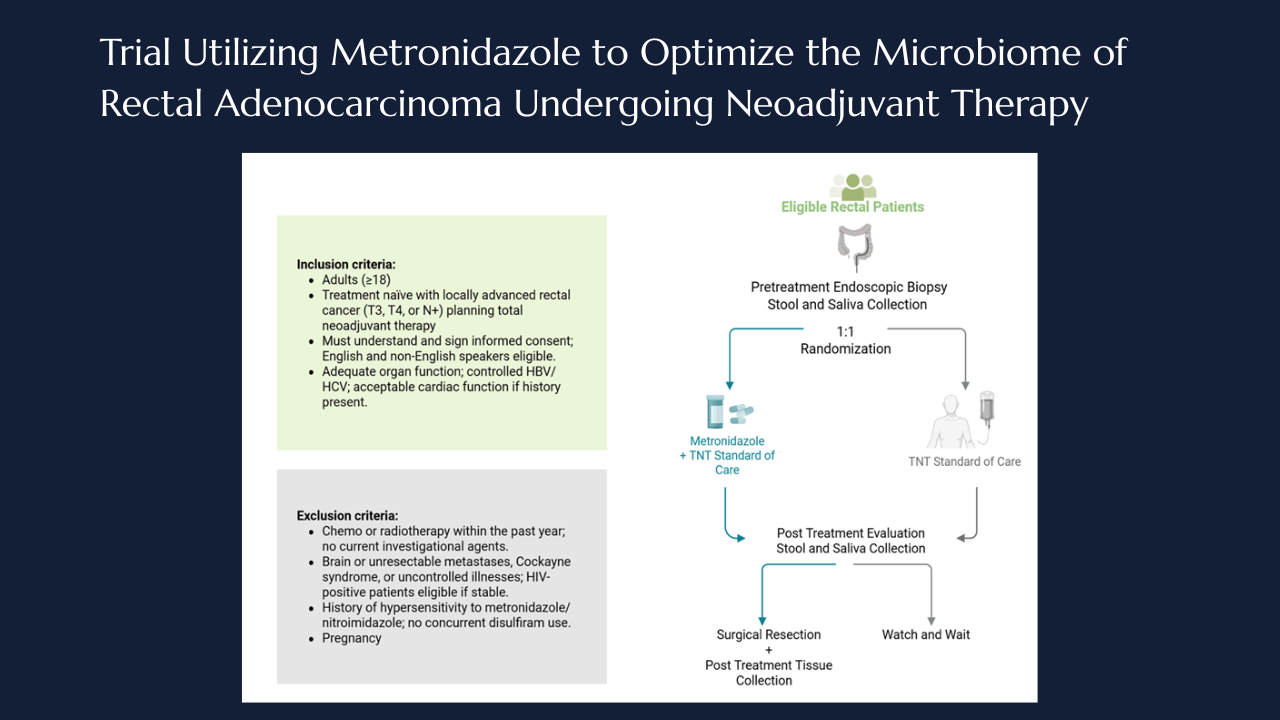
Targeting intratumoral microbiome: the MONARCH Trial takes aim at anaerobes in rectal cancer
Taylor M. Neilson, Laurence P. Diggs, Norman J. Galbraith, Jaganmurugan Ramamurthy, Neal Bhutiani, Ian Z. Hu, Arvind N. Dasari, Michael J. Overman, Scott E. Kopetz, Wei Qiao, Pranoti Sahasrabhojane, Vivian Orellana, Brian K. Bednarski, Montserrat Guraieb-Trueba, Ramy S. Behman, Ashish Damania, Nadim J. Ajami, Yan Wang, Mingxuan Xu, George J. Chang, Jennifer A. Wargo, Susan Bullman, Christopher D. Johnston, Y. Nancy You, Michael G. White

THrough knee AMputation’s impact on quality of Life compared to abovE knee ampuTation: THE HAMLET TRIAL
Sophie James , Sean Pymer , Catherine Arundel, Laura Doherty, Tom Davill, George Smith

Closing the treatment gap in knee osteoarthritis — the GEKO trial begins
Dr Raman Uberoi, Dr Anjali Shah, Dr Bhavisha Patel, Dr Loretta Davies, Professor Andrew Price, GEKO study group

The NEON trial: nerve repair vs. alignment for digital nerve injuries
Justin C R Wormald, MRCS, DPhil
Thank you to our strategic partners


.png)




Connect