



What's new
TOP ARTICLE
OF THE
MONTH
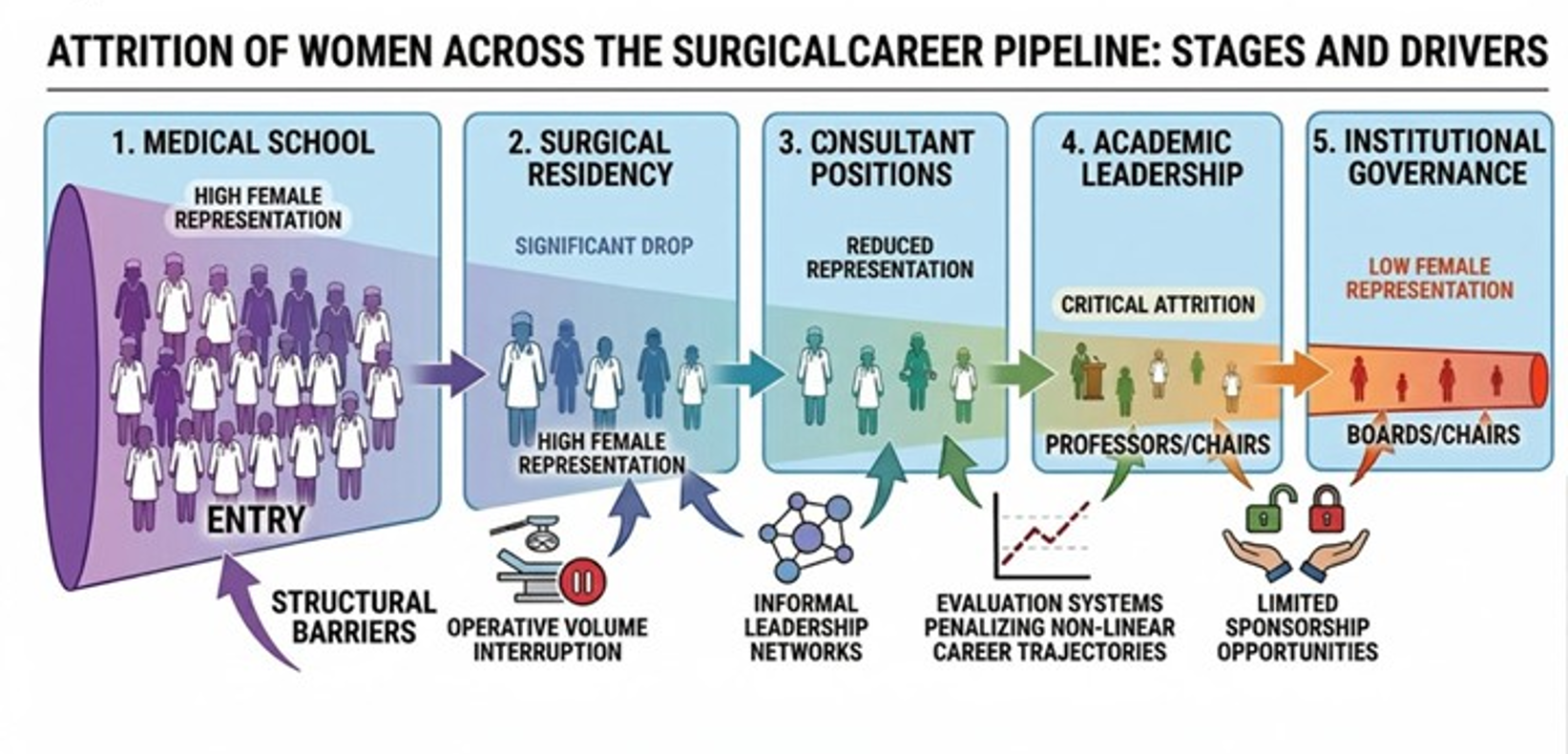
Remaining surgeons: pregnancy, sustainability, and institutional responsibility
RCT
OF THE
MONTH



JOIN
BJS Academy
Join BJS Academy And Receive Our Latest News And Updates.
Latest news and events





About
BJS Academy is an online educational resource for current and future surgeons. It serves as the home for all things relating to the BJS Foundation as well as produces content, both original and in conversation with material published in the BJS Journals.
BJS Academy was founded as a part of the charitable activity of BJS Foundation, which owns and operates the following.

A celebration of excellence in surgical science, the BJS Award recognises a discovery, innovation or scientific study that has changed clinical practice. Awarded every two years, this international accolade gives an exceptional individual the recognition they richly deserve.
Academy content is comprised of five distinct sections: Continuing surgical education, Young BJS, Cutting edge, Scientific surgery and Surgical news.


BJS Institute provides formal certified online surgical courses to surgeons in training and established surgeons who wish to develop their skills in surgical writing and publishing.

Championing a Partners collaborative approach, the Foundation offers two levels of partnership, each with their own unique benefits.
Thank you to our strategic partners


.png)




Connect