Continuing surgical education
As surgical science advances at an extraordinary rate, all surgeons have a duty to keep up to date to offer their patients treatment based on the latest research.
To support the professional development of general surgeons of all specialties, Continuing surgical education provides a wealth of formal digital courses, specialty digests and much more.
A myriad of skills and qualities are required to sustain a career in this field, including personal sacrifice, dedication and resilience. In this section, surgeons can access a series of publications exploring this important topic.




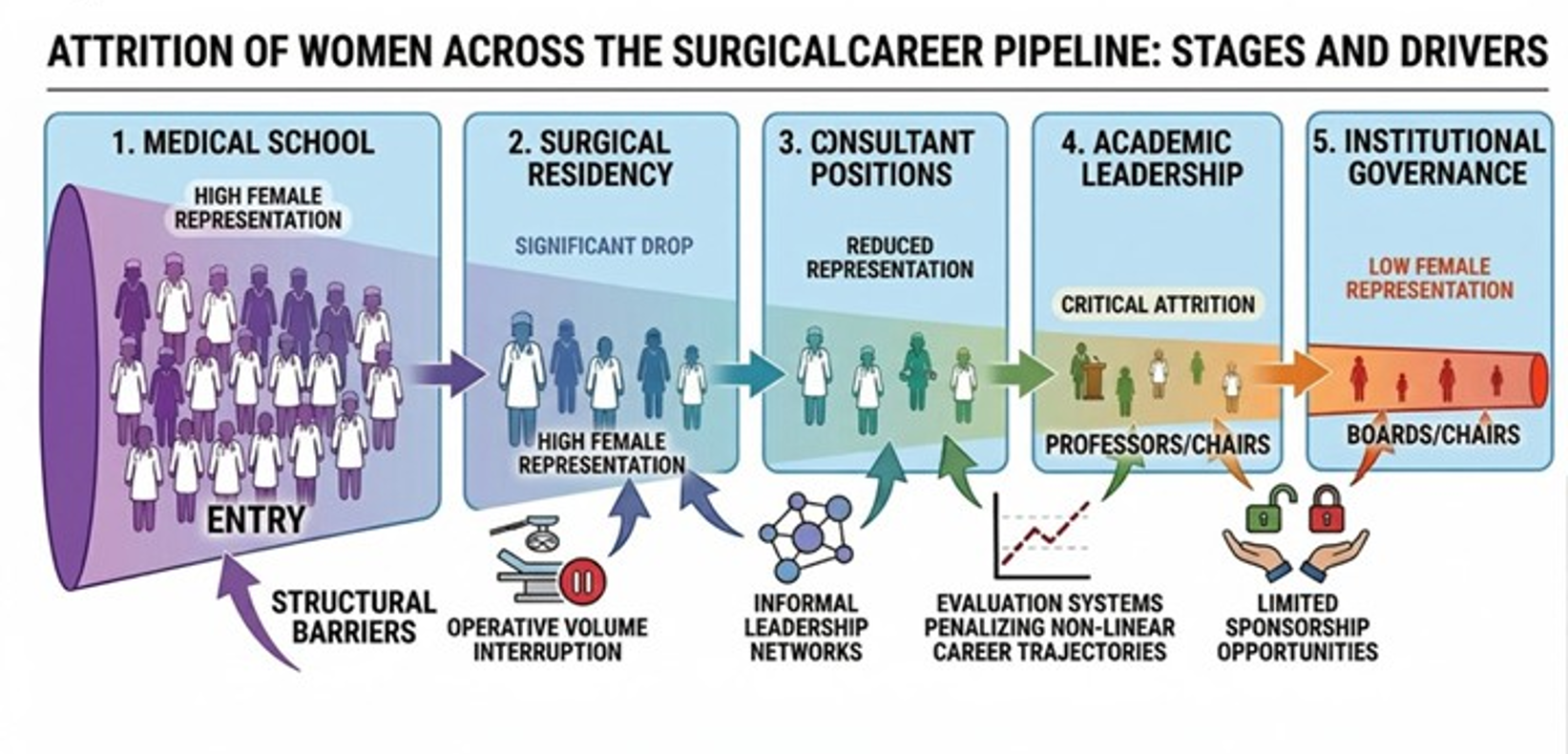
Remaining surgeons: pregnancy, sustainability, and institutional responsibility
Giulia Capelli, Dajana Glavas, Isabella Frigerio, Gaya Spolverato







Open Type II thoracoabdominal aortic aneurysm repair: key principles and operative insights
Mr Orwa Falah


Laparoscopic reduction of transverse colon and greater omentum from left chest, repair of giant para conduit/diaphragmatic hernia with mesh and colonopexy
Jubril O. Adigun, Shanmuga Kannan, Periyathambi Jambulingam, Othman Al-Fagih, Farhan Rashid
Thank you to our strategic partners


.png)




Connect