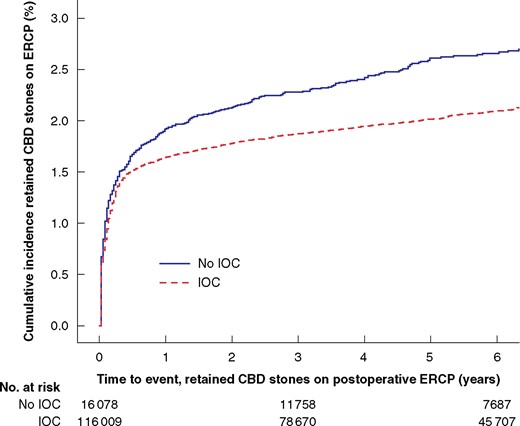
Each year 13 000 patients undergo cholecystectomy in Sweden, and routine intraoperative cholangiography (IOC) is recommended to minimize bile duct injuries. IOC plus an intervention to remove CBD stones identified during cholecystectomy was associated with reduced risk for retained stones and unplanned ERCP, even for the smallest asymptomatic CBD stones in this BJS study.
Normal View Dyslexic View
Video: Intervention versus surveillance in patients with common bile duct stones detected by intraoperative cholangiography
6 December 2021
Guest Blog HPB
Published on: 6 December 2021
Article ID: ce034
Related articles
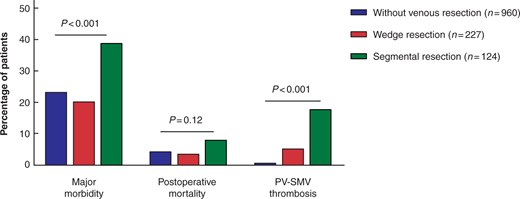
Guest blog: Venous resection during pancreatoduodenectomy – there is still much to gain
J.V. Groen, Department of Surgery, Leiden University Medical Centre, Leiden, J.V.Groen@lumc.nl N. Michiels, Department of Surgery, Leiden University Medical Centre, Leiden, N.Michiels@lumc.nl J.S.D. Mieog, Department of Surgery, Leiden University Medical Centre, Leiden, J.S.D.Mieog@lumc.nl

Guest blog: Death following pulmonary complications of surgery before and during the SARS-CoV-2 pandemic: how to compare apples and oranges?
Kenneth A McLean, Sivesh K Kamarajah, James C Glasbey
Thank you to our strategic partners


.png)





Connect