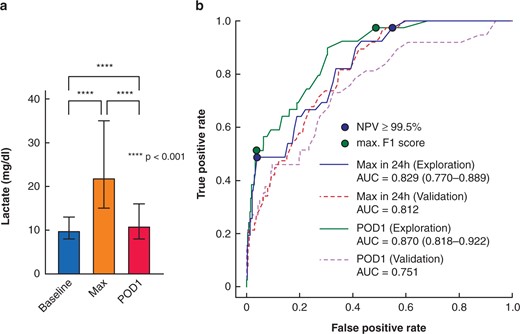
Post-hepatectomy liver failure (PHLF) represents the major determinant for death after liver resection. Early recognition is essential. Early postoperative lactate values are powerful, readily available markers for clinically relevant PHLF and associated complications after hepatectomy with potential for guiding postoperative care. This video explains the recent study published in BJS.
Normal View Dyslexic View
Video: Early postoperative arterial lactate concentrations to stratify risk of post-hepatectomy liver failure
6 December 2021
Guest Blog HPB
Published on: 6 December 2021
Article ID: ce033
Related articles
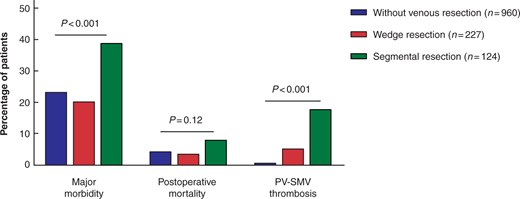
Guest blog: Venous resection during pancreatoduodenectomy – there is still much to gain
J.V. Groen, Department of Surgery, Leiden University Medical Centre, Leiden, J.V.Groen@lumc.nl N. Michiels, Department of Surgery, Leiden University Medical Centre, Leiden, N.Michiels@lumc.nl J.S.D. Mieog, Department of Surgery, Leiden University Medical Centre, Leiden, J.S.D.Mieog@lumc.nl

Guest blog: Death following pulmonary complications of surgery before and during the SARS-CoV-2 pandemic: how to compare apples and oranges?
Kenneth A McLean, Sivesh K Kamarajah, James C Glasbey
Thank you to our strategic partners


.png)





Connect