

N Husnoo
MJ Lee
Challenges of pregnancy
Caring for the pregnant woman with an acute abdomen is a particularly daunting challenge for the on-call surgeon. The surgeon is faced with concerns over the health of both the mother and foetus, bringing an emotive element to decision making. Assessment and diagnosis may be challenging for a number of reasons; the addition of obstetric-related diagnoses to the differential, displacement of anatomy by the gravid uterus, and challenges to the use of common diagnostic tools such as CT. In addition, the pregnant woman has altered physiology with increased circulating volume, decreased systemic vascular resistance, and a hyperdynamic state. This piece will discuss two common presentations, and some related considerations in care.
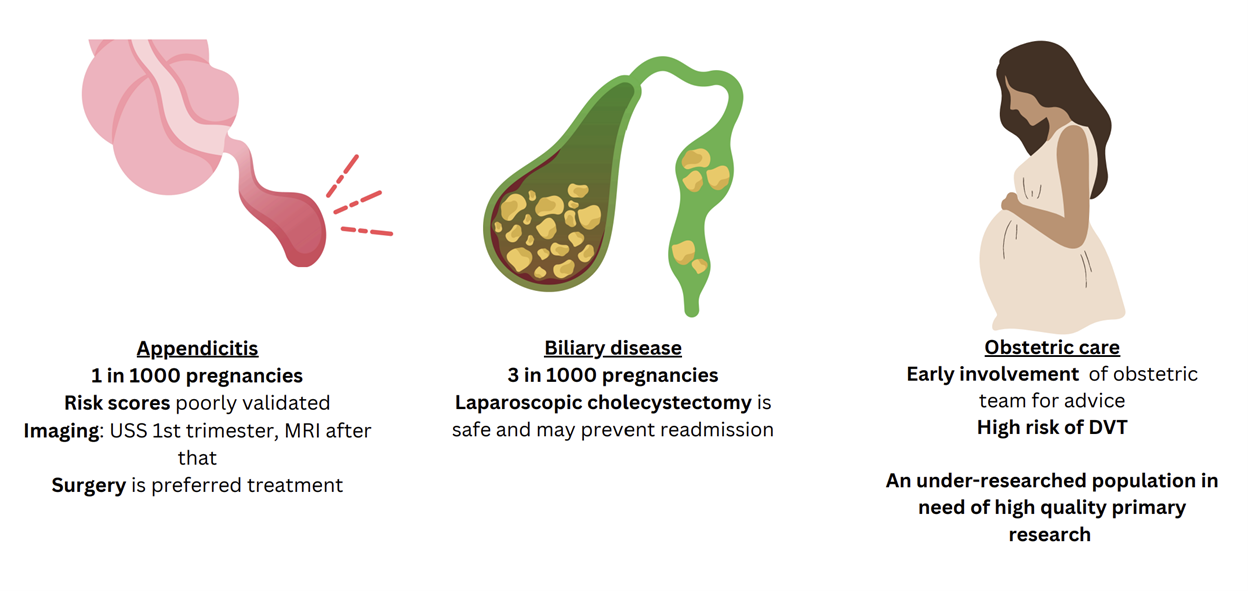
Figure 1: Key takeaways on common acute surgical conditions in pregnancy
Appendicitis
Acute appendicitis is thought to affect 1 in 1000 pregnancies.1, 2 Reaching an accurate diagnosis in a timely fashion remains a challenge in this cohort. Validation scores are derived from non-pregnant populations, and their performance has limited use.3 Aside from the difficulties in making a clinical diagnosis, the accuracy of imaging modalities is also affected by the gravid uterus. The accuracy of ultrasound scanning is low beyond the first trimester. Although magnetic resonance imaging (MRI) in this context is highly sensitive and specific, access to MRI can be highly variable across centres, especially out of hours, potentially leading to delays in initiating the appropriate treatment. The rate of non-visualisation with MRI is also higher in the 3rd trimester.4
The rate of foetal loss increases significantly in complex or perforated appendicitis ranging from 10-35%5-7 compared to simple appendicitis (<5%).7,8 Current guidelines3, 9, 10 support operative management of appendicitis in pregnancy, backed by evidence from large series highlighting the higher maternal and foetal morbidity associated with conservative management.1, 11 Despite this, recent literature shows that non-operative management is still common practice.12, 13 This may be a reflection of diagnostic difficulties, inconsistency in the evidence base and the surgeon’s reluctance to operate on the pregnant patient, compounded by knowledge that negative appendicectomy is associated with poor foetal outcomes.8
While American guidelines support a laparoscopic over an open approach to appendicectomy,12 UK guidelines do not recommend one approach over the other,9 based on evidence from a systematic review which demonstrated an increased risk of miscarriage associated with laparoscopic appendicectomy when compared to open.14 However, the adverse findings were influenced by a single large study.8 A large retrospective study subsequently also reported a higher risk of miscarriage with laparoscopic appendicectomy than with open, although the majority of its laparoscopic cases were performed in the first trimester.15 There is certainly a need for higher quality evidence in this area.
Biliary pathology
The incidence of gallstones in pregnancy ranges from 4.5 to 12%; symptomatic biliary disease occurs in 0.02 to 0.3% of pregnancies.16 As with non-pregnant patients, ultrasound scanning (USS) is highly accurate at establishing a diagnosis in cholelithiasis, with magnetic resonance cholangio-pancreatography being the imaging modality of choice where USS fails to confirm the diagnosis despite clinical or biochemical suspicion. Traditionally, non-operative management of symptomatic gallstone disease in pregnancy has been recommended. Current guidelines support early surgical management.3, 10 In uncomplicated disease (biliary colic), patients managed conservatively have a similar rate of preterm deliveries and foetal loss to patients managed surgically.17 There may be a role for supportive care, which is likely to lead to symptom resolution in most cases. However, the patient should be counselled about the high rates of recurrent biliary symptoms and subsequent hospitalisation with non-operative management,18 and the risk of ensuing complicated disease such as cholecystitis, acute pancreatitis and choledocholithiasis.
Cholecystitis and cholangitis may cause peritonitis and maternal sepsis, which are known to be associated with poor maternal and foetal outcomes. In a large series of 2719 patients, cholecystitis managed non-operatively was more likely to result in poor foetal growth, preterm delivery and a Caesarean section.19 Pancreatitis in pregnancy has historically been associated with significant maternal and foetal morbidity. Although this has now improved thanks to better diagnostic and treatment modalities, perinatal mortality was still noted to be 3.6% in a recent study.20 The highest rates of foetal loss and preterm delivery are observed in patients affected by pancreatitis during the first trimester.21
Although the evidence supports active surgical management of biliary disease, endoscopic and surgical procedures do have their own risks in the pregnant patient. In addition to the usual risks of an endoscopic retrograde cholangio-pancreatography (ERCP), the radiation effect of fluoroscopy may cause concern. However, radiation exposure of less than 50 mGy during pregnancy has not been shown to cause foetal anomalies. ERCP is associated with a foetal radiation exposure of around 0.40 mGy.22 As foetal radiation exposure is directly related to fluoroscopy time, only experienced clinicians should carry out this procedure in pregnant patients. Guidelines do support the judicious use of ERCP to manage symptomatic choledocholithiasis in pregnancy to prevent preterm labour or foetal loss.10
Laparoscopic cholecystectomy is also the treatment of choice for symptomatic gallstone disease regardless of the stage of pregnancy.3, 9 This recommendation is supported by findings, from a systematic review including 10,632 patients, of significantly lower foetal, maternal and surgical complications with laparoscopic compared to open cholecystectomy.23 However, in gallstone pancreatitis there may be benefit in delaying surgery to the 2nd trimester to reduce foetal morbidity ;3 laparoscopic cholecystectomy in the 3rd trimester can also be challenging due to reduced intra-abdominal space.
Stoma complications
One group worth of particular consideration is the pregnant woman who has a stoma due to IBD. A study of 82 pregnancies found significant stomarelated complications occurred during 1 in 4 pregnancies.24 This included stoma prolapse in 11%, of whom 22% required surgery. Parastomal hernia occurred in three pregnancies (3.5%), of whom two underwent surgery. Most notably, intestinal obstruction occurred in 8.5% of pregnancies, and half of these cases required surgical intervention. In this cohort 1 in 5 babies were delivered pre-term (<37 weeks).
Considerations in the management of the obstetric patient
A multidisciplinary team approach is key in this scenario that involves simultaneously caring for two patients. Depending on the stage of the pregnancy, this may involve a gynaecologist, an obstetrician, a neonatologist, a midwife and an obstetric anaesthetist, alongside the general surgeon. While the evidence increasingly supports a proactive surgical approach to the management of the acute abdomen, concerns about surgery causing potential harm to the foetus are high amongst both patients and clinicians. These need to be discussed thoroughly by the appropriate clinicians to allow the patient to make an informed decision.
Foetal considerations
Major embryonic development takes place in the first trimester. However, no clear link between anaesthetic agents and foetal teratogenesis has been found so far.25 A large series reporting outcomes of non-obstetric surgery (both abdominal and non-abdominal) found that although the overall rates of miscarriage and foetal death were low, these were increased when surgery was performed in the first trimester.5 The second trimester is usually preferred for non-urgent surgery that cannot be deferred to the postpartum period, as the risk for preterm delivery is at its lowest and surgical exposure is adequate with the uterus still lying in the lower abdomen. Foetal viability depends on uteroplacental blood flow and therefore intra-operative measures should be taken to avoid maternal hypotension and hypercapnia; it is recommended that insufflation pressure is limited to 12-15 mmHg at laparoscopy.26 Foetal heart Doppler ultrasound should be performed before and after surgery. After the age of foetal viability, surgery should ideally be undertaken in a unit that can provide obstetric and neonatal care in case delivery becomes necessary. If preterm delivery is a possibility, administration of antenatal corticosteroids for foetal lung maturation should be considered.
Maternal considerations
Obstetric patients with an acute intra-abdominal pathology are at an increased risk of venous thromboembolism. This risk increases with intra-abdominal surgery. The need for extended thromboprophylaxis should be considered.27 Intra-operatively, a left lateral tilt to avoid aortocaval compression by the gravid uterus should be considered. It should also be borne in mind that return to maternal physiological baseline is a gradual process that takes weeks, hence why it is recommended that elective surgery is postponed until at least six weeks postpartum.28
Summary
Management of the obstetric patient with an acute surgical abdomen is an area fraught with challenges. Non-obstetric abdominal conditions are uncommon and each general surgeon will only encounter them a handful of times in their career, making it difficult to build their individual experience. This is not helped by the fact that the evidence base consists purely of observational studies, mostly retrospective. The conduct of prospective studies would be impractical, and certainly randomised trials would be unethical. As a result, guidelines are based on low quality evidence, which may be one of the reasons that they are not always adhered to, leading to significant variations in practice. The decision-making around imaging and treatment can be complex and ideally warrants the input of the multidisciplinary team, which may not always be achievable depending on how local services are set up. There are multiple areas that warrant further research such as the optimal approach (conservative versus surgical or laparoscopic versus open) for various conditions in each trimester, and the sources and consequences of delays in making an accurate diagnosis. Standardised outcome-reporting will be key to building a more robust evidence-base. The creation of large national databases of surgical conditions in obstetric patients may be the most appropriate way of achieving this.
References
Abbasi N, Patenaude V, Abenhaim HA (2014) Management and outcomes of acute appendicitis in pregnancy-population-based study of over 7000 cases. BJOG 121:1509–1514
Mourad J, Elliott JP, Erickson L, Lisboa L (2000) Appendicitis in pregnancy: new information that contradicts long-held clinical beliefs. Am J Obstet Gynecol 182:1027–1029
Kenington JC, Pellino G, Iqbal MR, et al (2024) Guidelines on general surgical emergencies in pregnancy. Br J Surg 111:znae051
Theilen LH, Mellnick VM, Longman RE, et al (2015) Utility of magnetic resonance imaging for suspected appendicitis in pregnant women. Am J Obstet Gynecol 212:345.e1–6
Cohen-Kerem R, Railton C, Oren D, et al (2005) Pregnancy outcome following non-obstetric surgical intervention. Am J Surg 190:467–473
Ueberrueck T, Koch A, Meyer L, et al (2004) Ninety-four appendectomies for suspected acute appendicitis during pregnancy. World J Surg 28:508–511
Brown JJS, Wilson C, Coleman S, Joypaul BV (2009) Appendicitis in pregnancy: an ongoing diagnostic dilemma. Colorectal Dis 11:116–122
McGory ML, Zingmond DS, Tillou A, et al (2007) Negative appendectomy in pregnant women is associated with a substantial risk of fetal loss. J Am Coll Surg 205:534–540
Ball E, Waters N, Cooper N, et al (2019) Evidence-based guideline on laparoscopy in pregnancy: Commissioned by the British society for gynaecological endoscopy (BSGE) endorsed by the royal college of obstetricians & gynaecologists (RCOG). Facts Views Vis ObGyn 11:5–25
Pearl JP, Price RR, Tonkin AE, et al (2017) SAGES guidelines for the use of laparoscopy during pregnancy. Surg Endosc 31:3767–3782
Cheng H-T, Wang Y-C, Lo H-C, et al (2015) Laparoscopic appendectomy versus open appendectomy in pregnancy: a population-based analysis of maternal outcome. Surg Endosc 29:1394–1399
Nakashima M, Takeuchi M, Kawakami K (2021) Clinical outcomes of acute appendicitis during pregnancy: Conservative management and appendectomy. World J Surg 45:1717–1724
Yang J, Wen SW, Krewski D, et al (2021) Association of treatments for acute appendicitis with pregnancy outcomes in the United States from 2000 to 2016: Results from a multi-level analysis. PLoS One 16:e0260991
Wilasrusmee C, Sukrat B, McEvoy M, et al (2012) Systematic review and meta-analysis of safety of laparoscopic versus open appendicectomy for suspected appendicitis in pregnancy. Br J Surg 99:1470–1478
Balinskaite V, Bottle A, Sodhi V, et al (2017) The risk of adverse pregnancy outcomes following nonobstetric surgery during pregnancy: Estimates from a retrospective cohort study of 6.5 million pregnancies. Ann Surg 266:260–266
Ghumman E, Barry M, Grace PA (1997) Management of gallstones in pregnancy. Br J Surg 84:1646–1650
Date RS, Kaushal M, Ramesh A (2008) A review of the management of gallstone disease and its complications in pregnancy. Am J Surg 196:599–608
Othman MO, Stone E, Hashimi M, Parasher G (2012) Conservative management of cholelithiasis and its complications in pregnancy is associated with recurrent symptoms and more emergency department visits. Gastrointest Endosc 76:564–569
Rios-Diaz AJ, Oliver EA, Bevilacqua LA, et al (2020) Is it safe to manage acute cholecystitis nonoperatively during pregnancy?: A nationwide analysis of morbidity according to management strategy. Ann Surg 272:449–456
Eddy JJ, Gideonsen MD, Song JY, et al (2009) Pancreatitis in pregnancy. Obstet Anesth Dig 29:174
Tang S-J, Rodriguez-Frias E, Singh S, et al (2010) Acute pancreatitis during pregnancy. Clin Gastroenterol Hepatol 8:85–90
Kahaleh M, Hartwell GD, Arseneau KO, et al (2004) Safety and efficacy of ERCP in pregnancy. Gastrointest Endosc 60:287–292
Sedaghat N, Cao AM, Eslick GD, Cox MR (2017) Laparoscopic versus open cholecystectomy in pregnancy: a systematic review and meta-analysis. Surg Endosc 31:673–679
PAPooSE Study Group* (2022) Pregnancy outcomes after stoma surgery for inflammatory bowel disease: The results of a retrospective multicentre audit. Colorectal Dis 24:838–844
(2019) ACOG Committee opinion no. 775 summary: Nonobstetric surgery during pregnancy. Obstet Gynecol 133:844–845
O’Rourke N, Kodali B-S (2006) Laparoscopic surgery during pregnancy. Curr Opin Anaesthesiol 19:254–259
Thrombosis and Embolism during Pregnancy and the Puerperium, the Acute Management of. Royal College of Obstetricians and Gynaecologists
Nejdlova M, Johnson T (2012) Anaesthesia for non-obstetric procedures during pregnancy. Contin Educ Anaesth Crit Care Pain 12:203–206



.png)




