Introduction
With multiple advantages over laparoscopic and open surgery, including stereovision, enhanced precision and dexterity, surgeons are transitioning to robotic surgery. Practicing robotic surgeons praise the platform’s improved ergonomics and camera control, advantages that are worth the challenge of overcoming the steep learning curve.
Thus, robotics is becoming the cornerstone for advancing the field of minimally invasive surgery. An obvious pattern in the diffusion of cutting-edge technologies is that it starts with one manufacturer – Intuitive Surgical has currently near complete dominance of the robotic surgery market. However, in the future, new robotic platforms will become available. Here we discuss the advantages and challenges with robotic surgery.
Robotic surgery in numbers
In 2017, 877,000 robotic procedures were performed worldwide.1 Sheetz et al. reported an 8.4-fold increase of robotic general surgery procedures and a 0.8-fold decline in open surgery, from 2012 to 2018. Moreover, hospitals that adopted robotic procedures had a decrease in laparoscopic surgery from 53.2% to 51.3%, whereas a yearly increase by 1.3% was occurring for laparoscopic procedures before the adoption of robotic surgery.2 As of December 2021, a total of 6,526 robots provided by Intuitive Surgical are operational in 67 countries. Worldwide, 10 million robotic procedures have been performed.3
Advancement of the technology
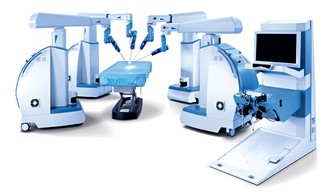
In the last five years, numerous companies around the world have invested in surgical robotics. Senhance, with clearance in the US, Europe, and Japan, offers a multiport-system consisting of four separate robotic arms in individual carts and an open console with a unique infrared eye-tracking system.
Figure 1 – Senhance Surgical System with its four separate robotic arms.
Revo-I is a four-arm patient cart with a closed console that received local clearance in Korea. The Versius platform consists of robotic arms individually mounted in portable carts and Avatera offers a patient cart and closed console, both receiving approval in Europe. Medicaroid developed Hinotori, the first robotic system to receive approval in Japan, which is composed of a surgeon cockpit, operative unit, and vision cart.
Figure 2 – The Hinotori surgical robot, approved for usage only in Japan.
Hugo from Medtronic received clearance in Europe in 2021. Additional systems such as Titan, a single port robotic platform from Canada, Bitrack, a three-arm open console with haptic feedback from Spain and the Tumai robot from China, are all competing to enter the market.4
Challenges and opportunities
Empowering the experts
Currently, about 55,000 robotic surgeons worldwide have been trained by Intuitive Surgical. A recent poll from the Robotic Surgery Collaboration (RSC) in December 2021 favored simulation as the method of training for the next decade. Intuitive Surgical offers a simulation learning program to surgeons who decide to venture into robotics: in 2020 the company provided a total amount of 34,000 training hours to 12,000 users, who performed 431,000 exercises on the system. There are over 1,100 registered proctors and the recent pandemic has forced many to consider virtual case observation and proctoring.
Figure 3 – Robotic simulation program from Intuitive Surgical, offers different settings for an optimal training.
Team Building and Mentorship
While robotic surgery somewhat offers autonomy to the surgeon, a competent OR team is critical. Team members have different levels of experience leading to a bell-curve-like team experience, most members in the middle and a small percentage being either beginners or masters. Thus, mentors should assemble members from all phases of the bell curve to guarantee success. Masters bring experience, rookies’ fresh perspectives and those in mid-bell enthusiasm and competence to run robotic surgery programs.
When training future robotic surgeons, many mentors find the robotic approach facilitating a clear stepwise fashion to operations which enables standardization of the workflow, potentially translating to improved quality of care.
Financial costs
Cutting-edge technology comes at a cost. However, one study found that overall costs in robotic versus laparoscopic surgery for rectal cancer were similar, even though mean operative costs for the robotic procedure were higher. Further, quality-adjusted life years were higher for robotic surgery.5 By the end of 2018, the global surgical robots’ market was estimated around $6.8 billion USD, with a prediction to reach $17 billion by 2025, nearly tripling in a span of 7 years.6 One new da Vinci Xi robotic system from Intuitive Surgical costs around $1.9 million.
Figure 4 – Vision Cart, Patient Cart, and Surgeon Console of a da Vinci Xi surgical robot.
Allocation for block utilization
Robotic allocation within the OR is a continually moving target. Administrators and surgeons across specialties must collaborate to improve utilization and efficiency. For most specialties, both robotic operating room times and robotic turnover times tend to be longer than for conventional procedures. Cohen, et al. found several remediable causes for this increased delay, such as non-productive time between different steps of turnover.7
Training the beginners: surgical education
Robotic surgery has a unique learning curve, both for novel and expert laparoscopic surgeons.8,9 Studies specifically investigating the learning curve in robotics showed a consistent and gradual decrease in operative time for robotic Rives-Stoppa ventral hernia repair after completing 29 cases, and improved outcomes after 51 cases.10 Similarly, the learning curve of robotic esophagectomy required at least 51 cases to achieve technical proficiency.11 To flatten the curve, surgeons should embrace fresher digital learning technologies that facilitate peer to peer collaboration and development.12 In this line, a recent study suggested that laparoscopic skills are transferrable to robotic surgery.13
Another innovation has been the development of bio-tissue-based simulation, or a combination of 3D-printing and hydrogel-casting technologies, yielding a fully immersive platform for robotic kidney transplantation training in a dry lab setting.14,15
The dual-console option in current robotic systems also aids teaching. Thus, residents are introduced to operating with the robot and taught to perform individual steps of the operation independently under a strict 4-eyes principle. The learning curve for young residents is fast and the system allows them to operate with the robot at an early stage.16 Didactically, robotic procedures can be divided into small steps, Entrustable Professional Activities (EPAs). These ensure patient safety, swift and timely operations, and a learning-friendly environment.17
Conclusion
Robotic surgery is headed for universal adoption. Robotics offers several advantages over traditional procedures. Given that robotics is still in its early stages compared to other modalities, the platform comes at the cost of higher operative expenses and a steeper learning curve. Healthy competition between robotic surgical companies and evolving training modalities will help overcome the mentioned challenges.
References
Childers, C. P. & Maggard-Gibbons, M. Estimation of the Acquisition and Operating Costs for Robotic Surgery. JAMA 320, 835–836 (2018).
Sheetz, K. H., Claflin, J. & Dimick, J. B. Trends in the Adoption of Robotic Surgery for Common Surgical Procedures. JAMA Netw. Open 3, 3–11 (2020).
Company, T., Systems, V. S., Company, T. & Company, T. Intuitive Announces Third Quarter Earnings. 2021, (2021).
Koukourikis, P. & Rha, K. H. Robotic surgical systems in urology: What is currently available? Investig. Clin. Urol. 62, 14–22 (2021).
Quijano, Y. et al. Robotic versus laparoscopic surgery for rectal cancer: a comparative cost-effectiveness study. Tech. Coloproctol. 24, 247–254 (2020).
Crew, B. A closer look at a revered robot. Nature 580, S5–S7 (2020).
Cohen, T. N. et al. Discovering the barriers to efficient robotic operating room turnover time: perceptions vs. reality. J. Robot. Surg. 14, 717–724 (2020).
Chandra, V. et al. A comparison of laparoscopic and robotic assisted suturing performance by experts and novices. Surgery 147, 830–839 (2010).
Yohannes, P., Rotariu, P., Pinto, P., Smith, A. D. & Lee, B. R. Comparison of robotic versus laparoscopic skills: is there a difference in the learning curve? Urology 60, 39–45; discussion 45 (2002).
Kudsi, O. Y. et al. Learning Curve of Robotic Rives-Stoppa Ventral Hernia Repair: A Cumulative Sum Analysis. J. Laparoendosc. Adv. Surg. Tech. 31, 756–764 (2021).
Han, Y. et al. Learning curve for robot-assisted Ivor Lewis esophagectomy. Dis. esophagus Off. J. Int. Soc. Dis. Esophagus (2021) doi:10.1093/dote/doab026.
Hachach-Haram, N. & Miskovic, D. Augmented Reality: Moving Robotics Forward. Clin. Colon Rectal Surg. 34, 345–352 (2021).
Kanitra, J. J. et al. Transference of skills in robotic vs. laparoscopic simulation: a randomized controlled trial. BMC Surg. 21, 379 (2021).
Feins, R. H. Real Tissue Robotic Simulation: The KindHeart Simulators. in Robotic Surgery (eds. Gharagozloo, F. et al.) 105–109 (Springer International Publishing, 2021). doi:10.1007/978-3-030-53594-0_10.
Saba, P. et al. Development of a High-Fidelity Robot-Assisted Kidney Transplant Simulation Platform Using Three-Dimensional Printing and Hydrogel Casting Technologies. J. Endourol. 34, 1088–1094 (2020).
Dietz, U. A. et al. Robotic hernia repair III. English version : Robotic incisional hernia repair with transversus abdominis release (r‑TAR). Video report and results of a cohort study. Chirurg. 92, 28–39 (2021).
Martin, L., Sibbald, M., Brandt Vegas, D., Russell, D. & Govaerts, M. The impact of entrustment assessments on feedback and learning: Trainee perspectives. Med. Educ. 54, 328–336 (2020).




.png)



