In 1985, Erich Mühe performed the first laparoscopic cholecystectomy. The German Surgical Society rejected him. Forty years later, a new systematic review asks: have we really learned how to evaluate surgical innovation?
The Story
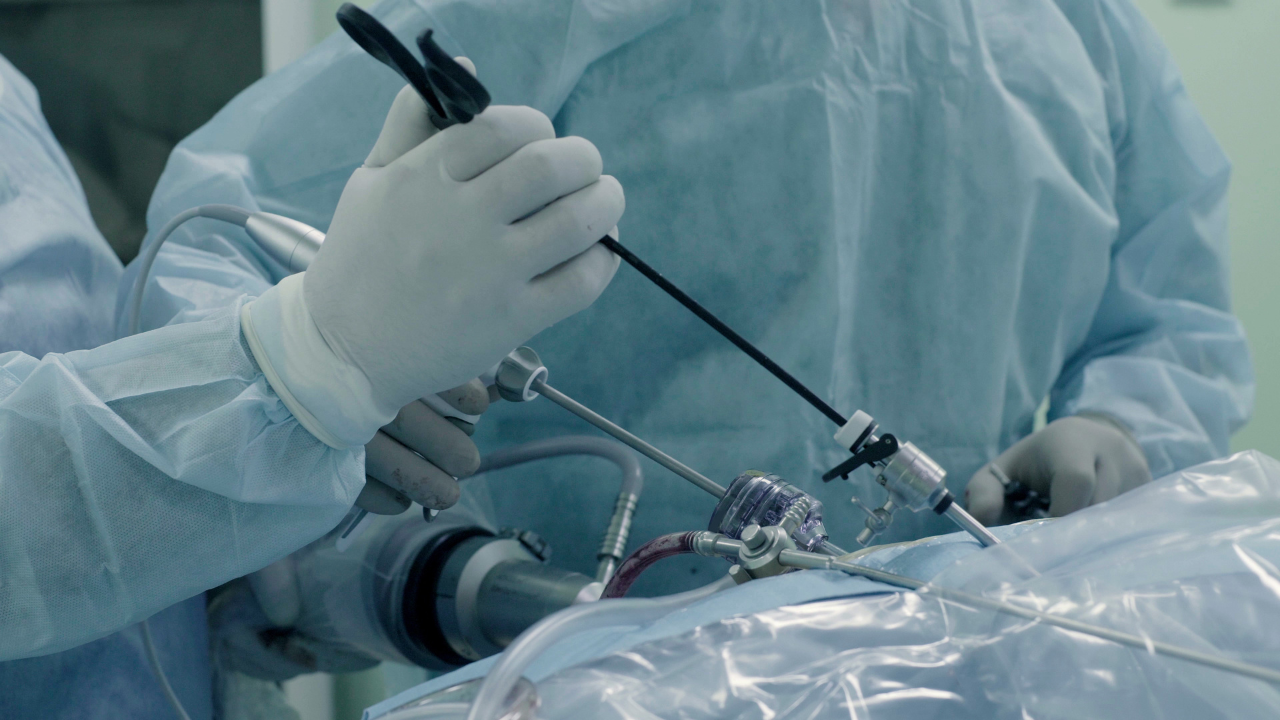
On September 12, 1985, Prof. Dr. Erich Mühe of Böblingen, Germany, performed the first laparoscopic cholecystectomy. By the time Mouret (1987) and Dubois (1988) had done their first, Mühe had already completed 94 cases.
When he presented his findings to the German Surgical Society in 1986, he was met not with curiosity but with skepticism, and was officially reprimanded.
Was the Society wrong? Yes and no.
Mühe was right about the innovation. He had done what he claimed. But 94 cases before any formal presentation, i.e. without prospective documentation, without a registered protocol, without the kind of staged evaluation we now expect, was an unusual path. The Society's skepticism, however poorly expressed, may have reflected an instinct that innovation needs oversight and not volume.
Mühe was eventually vindicated. He received the Society's highest award in 1992 and SAGES recognition in 1999. But his story reveals a persistent surgical dilemma: we have never known quite what to do with early innovation. We either attack the pioneer (Mühe) or allow innovation to proceed quietly for years without accountability.
Fast forward to 2026
In our new systematic review of non-standard metabolic bariatric procedures (DOI: 10.1093/bjs/znag047), we found the opposite problem. Not punishment for early reporting, but a gap in oversight.
Median publication lag: 5 years from first human operation to paper.
Prospective trial registration: Only 11%.
Long-term data (≥5 years): Just 14%.
High risk of bias: 98% of studies.
Over 10,000 patients underwent novel intestinal bypasses outside a transparent research framework. Perhaps someone should have asked: Where is the registry? Where is the long-term follow-up?
The crucial difference
Mühe operated in the 1980s, before modern research ethics frameworks existed for surgical innovation. His approach, to perform a series, then report it, was reasonable for his era.
Today, we have no excuse.
The IDEAL framework was published in 2009. It provides a clear, staged pathway from first-in-human cases (Stage 1) through development (Stage 2a), exploration (Stage 2b), assessment (Stage 3), and long-term study (Stage 4). It emphasizes prospective registration, transparent reporting, and methodical progression.
Our review1 spans 2000 to 2024. Among the 52 studies published after IDEAL, only 6 (12%) reported prospective trial registration. The framework exists, but we are not using it.
A way forward
The goal is not to judge Mühe by standards that did not yet exist. The goal is to hold ourselves, surgeons working in 2026, to the standards that do.
Journals: Make prospective registration a condition of publication for innovative procedures.
Societies: Link accreditation to IDEAL-aligned reporting.
Surgeons: Register early. The IDEAL framework is not a bureaucratic burden. It is the difference between pioneering with accountability and operating in the dark.
Mühe deserved better in 1986. Patients deserve better in 2026.
References
1.Papadia FS, De Cian O, Di Lorenzo N, Cohen RV. Navigating Uncharted Territory in Surgical Innovation: A systematic review of non-standard Metabolic Bariatric Surgery procedures. BJS 2026; doi: https://doi.org/10.1093/bjs/znag047



.png)



