Breast cancer is the most common cancer in women, and its incidence continues to increase worldwide. From the patient’s perspective, breast conserving surgery (BCS) with radiation achieves a balance between a satisfactory cosmetic result and a low recurrence rate. Although it has been established as a routine surgery, surgeons need to be careful about positive surgical margins. Remnant cancer cells in the preserved tissue increase the risk of recurrence. Therefore, a positive margin on postoperative pathology warrants additional surgery. In these cases, the additional treatment harbours unexpected outcomes, including physical, mental, cosmetic, and economic burden on the patients.
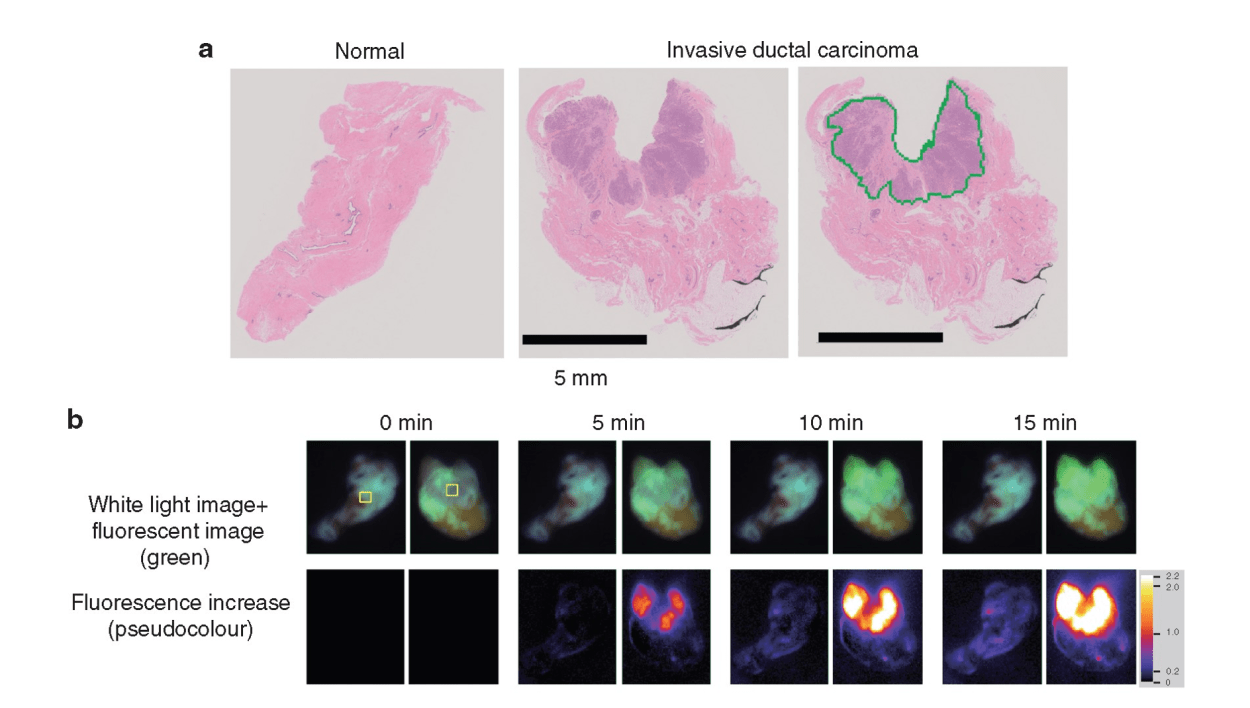
To avoid the additional operation, pathological evaluation using an intraoperative frozen section is conducted. It is the most reliable method to prevent misdiagnosis and to achieve clear surgical margins. However, this conventional method is time consuming and costly. Moreover, it is dependent on the skill and experience of the pathologists and personnel, and it requires space for preparation of the frozen sections. Therefore, only a limited number of samples are examined to save time and resources. An alternative, rapid, and reliable technique to detect cancer in surgical margins enables simultaneous testing, leading to a reduced false negative rate of local recurrence incidence. In addition, pathologists can focus on the definitive diagnosis using permanent paraffin sections because it is difficult to make a diagnosis based on intraoperative frozen sections without pathological architecture. Pathologists only need to make an intraoperative diagnosis when the specimen cannot be evaluated via the fluorescence procedure. Thus, it is important to enhance the rapid fluorescent detection of breast cancer during surgery. To address these diagnostic issues, Prof. Urano invented chemical reagents (gamma-glutamyl hydroxymethyl rhodamine green [gGlu-HMRG]) that quickly fluoresce by reacting with an enzyme (gamma-glutamyl transferase [GGT]), overexpressed in cancerous tissues. It exhibits strong fluorescence a few minutes after reacting with GGT in vitro. A gGlu-HMRG solution is applied to the surgical margins to recognize cancer cells as green fluorescence intraoperatively. A previous study in 2015 documented the ability of this reagent to mark cancerous tissues in surgical breast tissues. Furthermore, this reagent did not interfere with the pathological examination, while the frozen section analysis tissues were difficult to reuse as formalin-fixed and paraffin-embedded permanent pathological specimens.
The clinical utility of this technique was examined. The results were published in the British Journal of Surgery. Since the initial report in 2015, a more feasible and reproducible sample preparation protocol has been developed. Then, a dedicated apparatus, including a built-in camera, software programme, and multiple sample wells, was developed. This system automatically measured and analyzed the increase in fluorescence of multiple samples simultaneously. Then, the increase in fluorescence of gGlu-HMRG, applied to breast tissues, was measured in four different institutes. The sample tissues were examined by four pathologists independently. These pathologists diagnosed the samples without knowing the background information of the patients. The clinical utility of the current fluorescent procedure was evaluated by comparing the fluorescence data and the pathological diagnosis.
A clear threshold to distinguish between cancerous and non-cancerous tissues was not determined due to the heterogeneity of breast cancer tissues. Instead, the negative threshold to achieve a false negative rate <2% and the positive threshold to achieve a false positive rate <2% were established. Samples in which the increase in fluorescence was below the negative threshold value were considered cancer-free margins with a false negative rate <2%. The false negative samples in our study were tissues containing non-invasive cancer. This suggested that the samples below the negative threshold can be considered free of invasive cancer. Samples in which the increase in fluorescence was above the positive threshold value were considered cancerous tissue with a false positive rate <2%.
The disease prevalence determines the performance of a diagnostic tool. The percentage of positive and negative test results among those with or without the disease are the positive and negative predictive values, respectively. These positive and negative predictive values depended on the prevalence. Therefore, to estimate the performance of this technique, the prevalence and margin positive rate in this case should be considered. The margin positive rate was expectedly lower than that of our clinical study. In our protocol, three pieces of tissue were sampled: the central portion, where the breast cancer is located; its periphery, which contains non-invasive cancer; and the distal portion, which ideally contains normal mammary tissue. Cancer was detected in 46% of the samples. Based on the actual margin assessment, the prevalence was lower than that of our study. Assuming a prevalence <30%, the negative predictive value, the ratio of true negative samples among fluorescent negative samples, was larger than 98%. This indicated that this method was useful for detecting negative margins.
According to this multicenter study, the fluorescent diagnosis was applicable to any breast cancer subtype, regardless of its pathological findings and subtype. Moreover, the similar accuracy among several institutes confirmed that the fluorescent diagnosis was applicable to any institute, following the protocol. Compared to the intraoperative frozen section analysis, the fluorescent diagnosis was a more rapid and accessible method with a low cost. It was not dependent on the skills of pathologists, and it did not require a large amount of space.
In conclusion, this method can facilitate the rapid assessment of negative surgical margins during BCS while reducing the testing time, cost of diagnosis, and tasks of the pathologists and staff.





.png)



