Surgery is an indispensable part of health care, with about a third of the global burden of disease being surgical1. However, worldwide at least 4.8 billion people lack access to surgical care2, and surgery is estimated to account for a large proportion of preventable medical errors3.
Recent advances in artificial intelligence (AI) and Surgical Data Science4, bring with them the promise of a shift toward a more transparent, consistent, and democratized paradigm of surgical care. AI models trained to assess surgical quality, a practice today limited to research settings, could be used to extract quantitative information on performances at scale across procedures, greatly contributing to surgical transparency. Deployed in real-time, AI models could provide surgeons assistance in delivering the best possible care to patients, potentially increasing the quality of surgeries. Finally, replicating experts’ assessments, AI models could play a fundamental role in bringing knowledge where this is needed the most, hopefully democratizing access to high-quality surgery.
While level I evidence on the clinical benefits of diagnostic applications of AI is mounting, AI assistance in interventional healthcare is lagging, despite huge potential5. We attribute this lag to two factors specific to surgery. Firstly, modern operating rooms (ORs) are not natively fitted with the data acquisition and communication pipelines or the computation capabilities required to run commonly proposed AI models during procedures. Further, since surgery is one of the most high-stake, siloed, and conservative components of healthcare, a better understanding of the potential added value brought by AI is vital to gaining surgeons’ trust and uptake.
To address each of these concerns, we conducted an early-stage clinical evaluation of real-time AI assistance for laparoscopic cholecystectomy6.
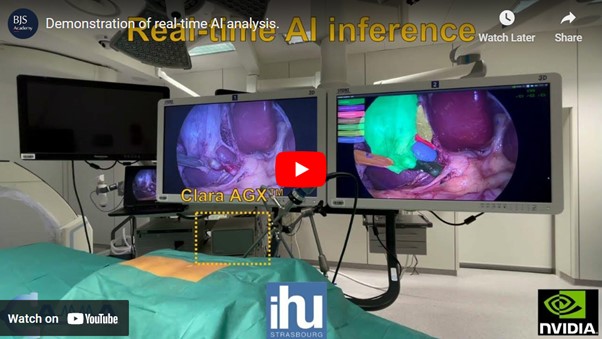
Technically, we have shown the feasibility of obtaining real-time predictions from several computationally expensive deep neural networks deployed in parallel on OR-ready hardware (Clara Holoscan, NVIDIA® Corporation, California, USA) provided in a research partnership.
SurgFlow, a toolkit of deep neural networks for surgical phase recognition7, tool tracking8, anatomical segmentation, and Critical View of Safety assessment9 developed by the CAMMA research group, was deployed in the experimental ORs of the Institute of Image-Guided Surgery (IHU-Strasbourg) to showcase the potential value of real-time AI assistance for laparoscopic cholecystectomy.
Surgeons and staff involved in the procedures as well as the vast audience that watched a live streaming of one of such AI-assisted laparoscopic cholecystectomies agreed that real-time AI predictions could serve different stakeholders in and around ORs, potentially improving the efficiency and safety of surgery.
We believe that this first early-stage clinical evaluation represents an important milestone in the quest to improve surgical care with real-time analytics. However, it is essential to achieve a better understanding of how to interface and integrate predictions into surgical workflows before advocating for the clinical translation of surgical AI. The journey toward AI-augmented operating rooms still necessitates a robust scientific, clinical, and technical effort, demanding collaboration from cross-disciplinary teams in academia and industry alike. These teams must work together to develop, validate, and integrate AI into interventional care
References
Meara JG, Leather AJM, Hagander L, Alkire BC, Alonso N, Ameh EA, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. The Lancet. Elsevier; 2015 Aug 8; 386: 569–624.
Alkire BC, Raykar NP, Shrime MG, Weiser TG, Bickler SW, Rose JA, et al. Global access to surgical care: a modelling study. The Lancet Global Health. Elsevier; 2015; 3: e316–e323.
Zegers M, de Bruijne MC, de Keizer B, Merten H, Groenewegen PP, van der Wal G, et al. The incidence, root-causes, and outcomes of adverse events in surgical units: implication for potential prevention strategies. Patient safety in surgery. Springer; 2011; 5: 13.
Maier-Hein L, Vedula SS, Speidel S, Navab N, Kikinis R, Park A, et al. Surgical data science for next-generation interventions. Nature Biomedical Engineering. Nature Publishing Group; 2017; 1: 691–696.
Maier-Hein L, Eisenmann M, Sarikaya D, März K, Collins T, Malpani A, et al. Surgical data science – from concepts toward clinical translation. Medical Image Analysis. 2022 Feb 1; 76: 102306.
Mascagni P, Alapatt D, Lapergola A, Vardazaryan A, Mazellier J-P, Dallemagne B, et al. Early-stage clinical evaluation of real-time artificial intelligence assistance for laparoscopic cholecystectomy. British Journal of Surgery. 2023 Nov 3; znad353.
Twinanda AP, Yengera G, Mutter D, Marescaux J, Padoy N. RSDNet: Learning to Predict Remaining Surgery Duration from Laparoscopic Videos Without Manual Annotations. IEEE Transactions on Medical Imaging. 2019 Apr; 38: 1069–1078.
Nwoye CI, Mutter D, Marescaux J, Padoy N. Weakly supervised convolutional LSTM approach for tool tracking in laparoscopic videos. Int J Comput Assist Radiol Surg. 2019 Jun; 14: 1059–1067.
Mascagni P, Vardazaryan A, Alapatt D, Urade T, Emre T, Fiorillo C, et al. Artificial Intelligence for Surgical Safety: Automatic Assessment of the Critical View of Safety in Laparoscopic Cholecystectomy Using Deep Learning. Annals of Surgery. 2022 May; 275: 955–961.



.png)



