IMPORTANCE
The use of venous resection (portal or superior mesenteric vein [PV-SMV]) during pancreatoduodenectomy is increasing.1-4 In a recent international survey, we found that most pancreatic surgeons prefer a segmental resection with primary anastomosis over a partial wedge resection, because of a lower perceived risk of complications.5 The impact of the type of venous resection (wedge or segmental) on postoperative morbidity and survival is poorly understood in current literature.
QUESTION
Does type of venous resection during pancreatoduodenectomy for pancreatic cancer impact postoperative morbidity and overall survival?
FINDINGS
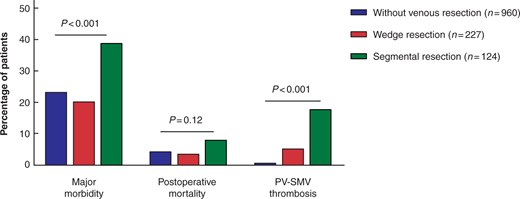
We performed a nationwide retrospective analysis of 1311 patients who underwent pancreatoduodenectomy for pancreatic cancer within the Dutch Pancreatic Cancer Group (2013-2017). A venous resection was performed in 27% patients (65% wedge resection; 35% segmental resection). Patients with segmental resection had more Clavien-Dindo ≥III complications (adjusted odds ratio 1.90, 95% confidence interval 1.22-2.98) and worse survival (adjusted hazard ratio 1.40, 95% confidence interval 1.10-1.78) compared to no venous resection. Patients with segmental resection had a higher rate of PV-SMV thrombosis (18%) as compared to patients with wedge resection (5%) and without venous resection (1%). Vascular complications (PV-SMV thrombosis or haemorrhage) were the indication for relaparotomy in 18 out of 23 (78%) patients with segmental resection. Tumour invasion in the resected PV-SMV did not differ between patients with segmental (67%) or wedge resection (69%).
In patients treated with neoadjuvant therapy, survival was comparable between types of venous resection, although patients with segmental resection had more Clavien-Dindo ≥III complications (52%) compared to venous wedge (19%) and without venous resection (21%).
MEANING
In contrast with the found preference for a segmental resection in the international survey, most patients underwent a wedge resection. Little is known what exactly drives the surgeon’s preference regarding choice of type of venous reconstruction.5 The results of this study implicate that an upfront segment resection is associated with both poor postoperative morbidity and poor survival. These findings are in line with a recent large international cohort study6 and contribute to the growing evidence that neoadjuvant chemotherapy should be considered in borderline resectable disease and suspected venous involvement.
FUTURE
This study, and other studies from our group5,7, on venous resection during pancreatoduodenectomy demonstrated that there is much to gain with regards to patient selection (~30% of patients with venous resection do not have tumour invasion in the resected PV-SMV), surgical technique (variation in clamping techniques, heparinization, types of reconstruction and use of grafts and flow measurements), postoperative management (e.g. vascular complications as PV-SMV thrombosis, haemorrhages and portal hypertension) and pathological assessment (lack of internationally accepted grossing techniques of venous resections). We believe this is especially relevant for the future since venous resection will be even more common with the increasing use of neoadjuvant therapy.
Several imaging tools are being investigated which can help selecting the right patients who need a venous resection to achieve a radical resection. Intraoperative ultrasound provides real-time imaging and feedback about the tumour, vascular involvement and resectability in patients with pancreatic cancer.8,9 We are currently analysing the data of our ULTRAPANC study which assesses the added value of intraoperative ultrasound in patients with pancreatic cancer and vascular involvement (https://www.trialregister.nl/trial/7621). A recent study showed the utility of computed tomography coupled with 3-dimensional image reconstruction in the assessment of superior mesenteric artery involvement after neoadjuvant therapy, the authors distinguish a “halo sign” (not involved) from a “string sign” (involved).10 An interesting topic would be if these ‘’halo and string signs’’, are also useful in the assessment of venous involvement with intraoperative ultrasound (or analogous ‘’signs’’, as the venous wall does not have an tunica adventitia).
Recently defined benchmark outcomes for pancreatoduodenectomy with venous resection can be used to assess outcomes and identify areas for improvement on a hospital, regional or national level.11 The PREOPANC-4 trial (protocol in preparation) within the Dutch Pancreatic Cancer Group will investigate the implementation of a best-practice algorithm for patients with locally advanced pancreatic cancer. This study has the potential to improve surgical technique and management of patients undergoing arterial/venous resection during pancreatoduodenectomy in the Netherlands.
In the present study, no data were available on the diagnosis, treatment and outcome of patients with PV-SMV thrombosis. We are currently collecting data for a successive study in which we will provide an overview of the current clinical practice in the Netherlands regarding the prevention, diagnosis, treatment and outcome of PV-SMV thrombosis following venous resection during pancreatoduodenectomy. A group from Japan recently performed an impressive study among 40 centres which showed that venous resection during pancreatoduodenectomy with splenic vein division frequently causes variceal formation, bleeding, and thrombocytopenia.12
Within the Dutch Pancreatic Cancer Group, pathological assessment of venous involvement have recently been standardized. The location of deepest invasion in the resected PV-SMV is assessed and all edges of the resected PV-SMV are assessed for radicality. A prospective study with this standardized pathological assessment is needed in to investigate the true prognostic value of (depth of) tumour invasion in the resected PV-SMV.
References
Kantor O, Talamonti MS, Wang CH, Roggin KK, Bentrem DJ, Winchester DJ, Prinz RA, Baker MS. The extent of vascular resection is associated with perioperative outcome in patients undergoing pancreaticoduodenectomy. HPB (Oxford) 2018;20(2): 140-146.
Kleive D, Sahakyan MA, Berstad AE, Verbeke CS, Gladhaug IP, Edwin B, Fosby B, Line PD, Labori KJ. Trends in indications, complications and outcomes for venous resection during pancreatoduodenectomy. Br J Surg 2017;104(11): 1558-1567.
van Roessel S, Mackay TM, Tol J, van Delden OM, van Lienden KP, Nio CY, Phoa S, Fockens P, van Hooft JE, Verheij J, Wilmink JW, van Gulik TM, Gouma DJ, Busch OR, Besselink MG. Impact of expanding indications on surgical and oncological outcome in 1434 consecutive pancreatoduodenectomies. HPB (Oxford) 2019;21(7): 865-875.
Worni M, Castleberry AW, Clary BM, Gloor B, Carvalho E, Jacobs DO, Pietrobon R, Scarborough JE, White RR. Concomitant vascular reconstruction during pancreatectomy for malignant disease: a propensity score-adjusted, population-based trend analysis involving 10,206 patients. JAMA Surg 2013;148(4): 331-338.
Groen JV, Stommel MWJ, Sarasqueta AF, Besselink MG, Brosens LAA, van Eijck CHJ, Molenaar IQ, Verheij J, de Vos-Geelen J, Wasser MN, Bonsing BA, Mieog JSD, Dutch Pancreatic Cancer G. Surgical management and pathological assessment of pancreatoduodenectomy with venous resection: an international survey among surgeons and pathologists. HPB (Oxford) 2021;23(1): 80-89.
Machairas N, Raptis DA, Velázquez PS, Sauvanet A, de Leon AR, Oba A, Koerkamp BG, Lovasik B, Chan C, Yeo C, Bassi C, Ferrone CR, Kooby D, Moskal D, Tamburrino D, Yoon DS, Barroso E, de Santibañes E, Kauffmann EF, Vigia E, Robin F, Casciani F, Burdío F, Belfiori G, Malleo G, Lavu H, Hartog H, Hwang HK, Han HS, Marques HP, Poves I, Rosado ID, Park JS, Lillemoe KD, Roberts K, Sulpice L, Besselink MG, Abuawwad M, Del Chiaro M, de Santibañes M, Falconi M, D'Silva M, Silva M, Hilal MA, Qadan M, Sell NM, Beghdadi N, Napoli N, Busch OR, Mazza O, Muiesan P, Müller PC, Ravikumar R, Schulick R, Powell-Brett S, Abbas SH, Mackay TM, Stoop TF, Gallagher TK, Boggi U, van Eijck C, Clavien PA, Conlon KCP, Fusai GK. The Impact of Neoadjuvant Treatment on Survival in Patients Undergoing Pancreatoduodenectomy with Concomitant Portomesenteric Venous Resection: An International Multicenter Analysis. Ann Surg 2021.
Groen, Jesse V. MD∗; van Manen, Labrinus MD∗; van Roessel, Stijn MD, PhD†; van Dam, Jacob L. MD‡; Bonsing, Bert A. MD, PhD∗; Doukas, Michael MD, PhD§; van Eijck, Casper H.J. MD, PhD‡; Farina Sarasqueta, Arantza MD, PhD∥; Putter, Hein MD, PhD¶; Vahrmeijer, Alexander L. MD, PhD∗; Verheij, Joanne MD, PhD∥; Besselink, Marc G. MD, PhD†; Groot Koerkamp, Bas MD, PhD‡; Mieog, J. Sven D. MD, PhD∗ Resection of the Portal-Superior Mesenteric Vein in Pancreatic Cancer, Pancreas: September 2021 - Volume 50 - Issue 8 - p 1218-1229 doi: 10.1097/MPA.0000000000001897
Sibinga Mulder BG, Feshtali S, Farina Sarasqueta A, Vahrmeijer AL, Swijnenburg RJ, Bonsing BA, Mieog JSD. A Prospective Clinical Trial to Determine the Effect of Intraoperative Ultrasound on Surgical Strategy and Resection Outcome in Patients with Pancreatic Cancer. Ultrasound Med Biol 2019;45(8): 2019-2026.
van Veldhuisen E, Walma MS, van Rijssen LB, Busch OR, Bruijnen RCG, van Delden OM, Mohammad NH, de Hingh IH, Yo LS, van Laarhoven HW, van Leeuwen MS, Nio CY, van Santvoort HC, de Vries J, Wessels FJ, Wilmink JW, Molenaar IQ, Besselink MG, van Lienden KP, Dutch Pancreatic Cancer G. Added value of intra-operative ultrasound to determine the resectability of locally advanced pancreatic cancer following FOLFIRINOX chemotherapy (IMAGE): a prospective multicenter study. HPB (Oxford) 2019.
Habib JR, Kinny-Köster B, van Oosten F, Javed AA, Cameron JL, Lafaro KJ, Burkhart RA, Burns WR, He J, Thompson ED, Fishman EK, Wolfgang CL. Periadventitial dissection of the superior mesenteric artery for locally advanced pancreatic cancer: Surgical planning with the "halo sign" and "string sign". Surgery 2020.
Raptis DA, Sánchez-Velázquez P, Machairas N, Sauvanet A, Rueda de Leon A, Oba A, Groot Koerkamp B, Lovasik B, Chan C, Yeo CJ, Bassi C, Ferrone CR, Kooby D, Moskal D, Tamburrino D, Yoon DS, Barroso E, de Santibañes E, Kauffmann EF, Vigia E, Robin F, Casciani F, Burdío F, Belfiori G, Malleo G, Lavu H, Hartog H, Hwang HK, Han HS, Poves I, Rosado ID, Park JS, Lillemoe KD, Roberts KJ, Sulpice L, Besselink MG, Abuawwad M, Del Chiaro M, de Santibañes M, Falconi M, D'Silva M, Silva M, Abu Hilal M, Qadan M, Sell NM, Beghdadi N, Napoli N, Busch ORC, Mazza O, Muiesan P, Müller PC, Ravikumar R, Schulick R, Powell-Brett S, Abbas SH, Mackay TM, Stoop TF, Gallagher TK, Boggi U, van Eijck C, Clavien PA, Conlon KCP, Fusai GK. Defining Benchmark Outcomes for Pancreatoduodenectomy With Portomesenteric Venous Resection. Ann Surg 2020;272(5): 731-737.
Mizuno S, Kato H, Yamaue H, Fujii T, Satoi S, Saiura A, Murakami Y, Sho M, Yamamoto M, Isaji S. Left-sided Portal Hypertension After Pancreaticoduodenectomy With Resection of the Portal Vein/Superior Mesenteric Vein Confluence in Patients With Pancreatic Cancer: A Project Study by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. Ann Surg 2021;274(1): e36-e44.



.png)




