Introduction
Oesophageal cancer ranks seventh in terms of incidence and sixth in mortality overall, being responsible for one in every 18 cancer deaths in 2020 worldwide1. There are two main histological types: squamous cell carcinoma and adenocarcinoma. The overall 5-year survival of patients diagnosed with oesophageal cancer is approximately 15%2. Apart from some areas in Asia, there is no screening programme worldwide. Hence, patients often present with advanced disease stage and cure is seldom possible. Some 50-60% of patients can be offered treatment with curative intent including surgical and non-surgical modalities3. Disease stage, patient’s fitness/frailty and expertise of the multidisciplinary team guide decision making.
Anatomy of the oesophagus (figure 1)
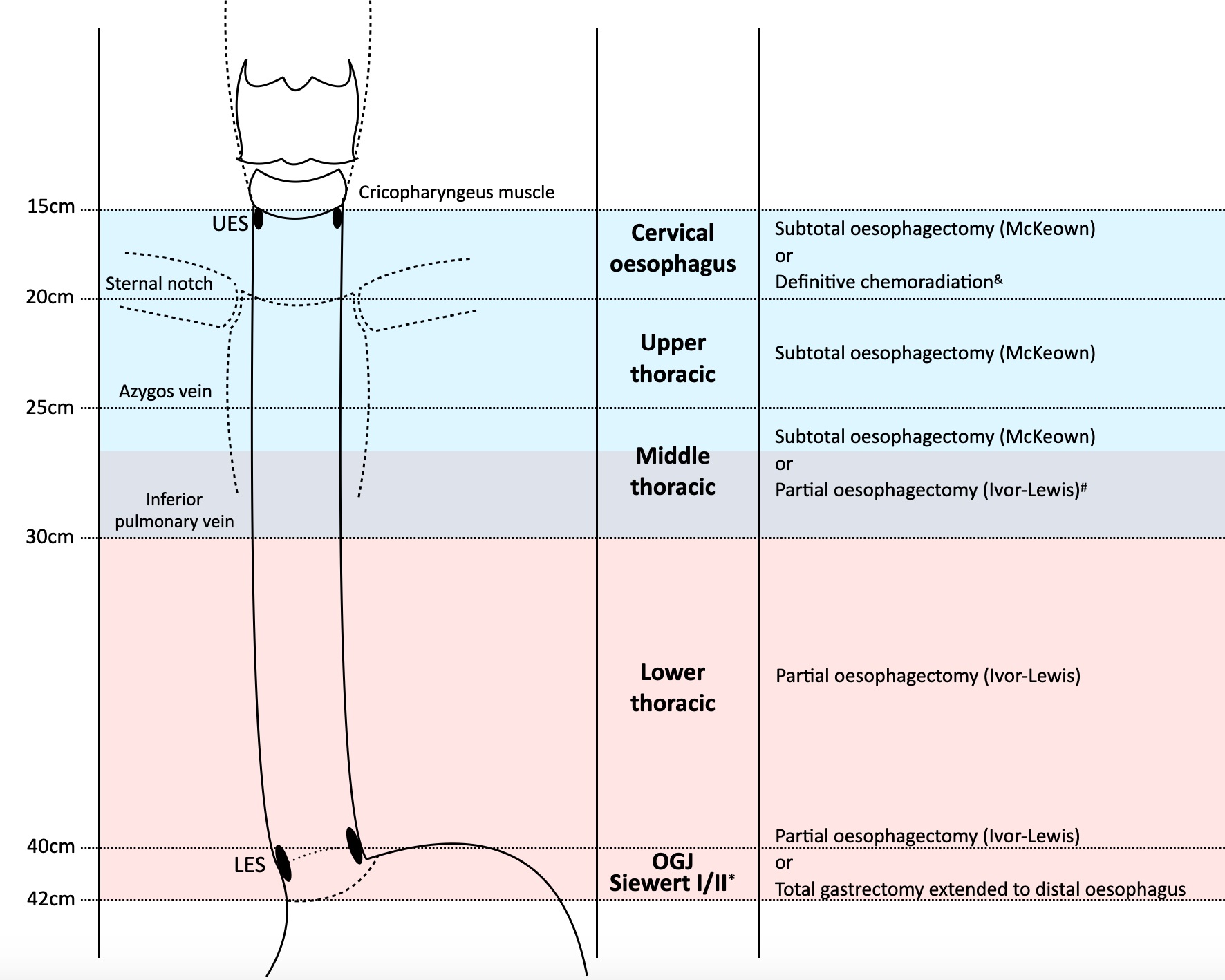
Figure 1. Recommended oesophageal resections according to the location of the tumour. *The preferred surgical treatment for Siewert type I is partial oesophagectomy with transthoracic mediastinal lymph node dissection, but for type II both partial oesophagectomy with mediastinal lymph node dissection or total gastrectomy with extension of the resection to the distal oesophagus may be valid.&Cervical or cervicothoracic oesophageal carcinomas less than 3-5cm from the cricopharyngeus should be treated with definitive chemoradiation.#A proximal safe resection margin of at least 3.5-5cm must be ensured for a complete resection (R0) and to decrease the risk of local recurrence.
The oesophagus is a 25 cm long fibromuscular tube extending from the hypopharynx to the stomach. It lies posterior to the trachea and the heart and passes through the mediastinum and the hiatus in its descent from the chest to the abdomen. It is subdivided into three segments related to anatomical boundaries. Typical endoscopic measurements of each region measured from the incisors depend on body size and height4,5:
Cervical oesophagus: begins at the lower end of pharynx (level of 6th vertebra or lower border of cricoid cartilage) and extends to the thoracic inlet (suprasternal notch); 18-20cm from incisors.
Thoracic oesophagus: the oesophagus in the thoracic cavity:
Upper thoracic: from thoracic inlet to lower border of the azygos vein; from 18-20cm to 23-25cm.
Middle thoracic: from lower border of the azygos vein to lower border of the inferior pulmonary vein; from 23-25cm to 30-32cm.
Lower thoracic: from lower border of the inferior pulmonary vein to the stomach, including the oesophagogastric junction; from 30-32cm to 40-42cm.
– Abdominal oesophagus: part of lower thoracic oesophagus, it involves the OGJ positioned at the diaphragm/upper abdomen; 40-42cm.
The oesophagogastric junction (OGJ) is the region where the oesophagus joins the stomach. The gastric cardia is the area of mucosa distal to the OGJ and proximal to the oxyntic mucosa of the gastric body, also known as cardiac orifice (the opening of the oesophagus into the stomach). The location of oesophageal cancer is defined by the epicenter of the tumour. According to the Siewert classification, a cancer of the OGJ is defined as a tumour whose epicenter is located within 5 cm proximal and distal of the OGJ. Siewert type I indicates an epicenter 1-5 cm above the OGJ; type II (cardia cancer) with a center within 1 cm above and 2 cm below OGJ; type III center 2-5 cm below the OGJ. Siewert types I and II are staged according to the TNM-system of oesophageal cancers whereas type III, even if the OGJ is involved, are staged according to the principles of gastric cancer.
Diagnostic work-up and staging
Oesophageal cancer is often categorized as early (cT1-T2 N0 M0), locally advanced (cT3-T4 and/or cN1-N3 M0) or metastatic disease (M1) (see Table 1). Clinical staging involves an upper GI endoscopy. The upper and lower border of the tumour (in relation to the incisors), traversibility, and other important landmarks (Z-line, gastric folds, impression of diaphragm) are carefully registered. Multiple biopsies are taken from the tumour for histological assessment. Histological type (adenocarcinoma, squamous cell carcinoma and others) and grade of differentiation are reported by the pathologist. Endoscopic ultrasound (EUS) +/- fine needle aspiration (FNA) of suspicious lymph nodes has the highest accuracy for T- and N-staging. A high resolution CT-chest-abdomen with intravenous contrast is mandatory to assess the relation of the tumour with surrounding anatomical structures and locoregional and distant nodal or organ metastases. A full body PET-CT scan is routinely performed to exclude distant metastases. If the tumour is located at or above the level of the carina, a tracheobronchoscopy should be performed to exclude invasion of the tracheobronchial tree as this influences the plan of treatment. For oesophageal squamous cell carcinoma (SCC), assessment of the patient by an ear, nose and throat (ENT) specialist should be considered to exclude a second primary tumour of the upper aerodigestive tract given common risk factors (tobacco and alcohol).
Table 1. TNM categories and clinical staging of oesophagus and oesophagogastric junction cancer, according to AJCC Cancer Staging Manual, 8th edition3
Surgical treatment
Oesophagectomy carries a risk of death within 90-days after surgery in the order of 5%. Postoperative complications are seen in 60% of patients6. Indications for surgical resection should be discussed and agreed by a multidisciplinary tumour board (MTB) including an oesophagogastric surgeon, medical oncologist, radiotherapist, radiologist, pathologist and gastroenterologist. When oesophagectomy is considered the best treatment option, the patient’s fitness for surgery should be carefully assessed, balancing the risks and benefits of surgery for the individual with the aim to obtain the best outcome in terms of survival and quality of life (QOL).
Tumours located at least 3-5cm from the cricopharyngeus muscle (UES) up to and including the OGJ (Siewert I-II) should be considered for oesophagectomy. Cervical or cervicothoracic oesophageal carcinomas are preferably treated with definitive chemoradiation (dCRT) as laryngo-pharyngo-esophagectomy with a tracheostomy is otherwise needed in these patients, which carries a considerable high risk along with a very significant morbidity over speech and swallowing functions7.
Early-stage cancer
For early-stage disease (pTis-T1am1/m2N0 squamous cell carcinoma, or superficial pT1a-T1bsm1N0 adenocarcinoma) with histological low risk features (no lymphovascular invasion, well or moderately differentiated carcinoma, diameter ≤2cm, no ulceration) endoscopic resection is often the treatment of first choice given the organ sparing character, lower treatment-related morbidity and better quality of life8-10.
Locally advanced cancer
Patients with limited locoregional (cT1-T2 cN0 M0) and locally advanced (cT3-T4a or cN1-3 M0) disease are considered candidates for surgery. Tumours with organ metastases and non-regional lymph node involvement, OGJ tumours with supraclavicular lymph node involvement, and T4b tumours with involvement of the heart, great vessels, trachea, vertebrae or adjacent organs including liver, pancreas and spleen are considered unresectable and incurable8-10.
Primary oesophagectomy has been the standard for many decades. Historically, a fair proportion of patients had tumour-positive resection margins (R1) and overall survival was only 35-40%. Preoperative chemotherapy or chemo-radiotherapy was introduced to minimize the risk of irradical resections and to decrease the development of locoregional and/or distant recurrences. Neoadjuvant chemotherapy or chemoradiotherapy followed by oesophagectomy improve overall survival as compared to surgery alone without a substantial impact on postoperative morbidity and mortality11,12. Currently, controversy exist regarding which therapy is superior. Radiotherapy aims to maximize locoregional disease control while chemotherapy has the potential to eliminate micrometastases. However, no robust evidence on the optimal neoadjuvant treatment has been obtained as yet. Large randomized controlled trials like the Neo-AEGIS-II and ESOPEC are now addressing this topic13.
Non-surgical treatment
Definitive chemo-radiotherapy (dCRT) has been reserved for those patients who are deemed unsuitable for surgery due to poor performance status, comorbidities and/or extent of disease (cT4b), and also for those unwilling to undergo oesophagectomy. It achieves survival rates of 35–40% at 2 years and about 20% at 5 years, although with higher rates of local recurrence and persistent disease compared to multimodal therapy7,14. Particularly, SCC histology and stage I disease respond favourable to dCRT (3-year survival rate up to 42%)14. It is a good alternative in frail and elderly patients15, in whom oesophagectomy would lead to unacceptable high morbidity and mortality. As discussed earlier, dCRT is recommended for cervical oesophageal carcinomas. The outcomes of dCRT in cervical oesophageal cancer are comparable to upfront surgery, but with the significant advantage of preservation of laryngeal organ function, such as speech and swallowing. Distant metastasis, rather than local recurrence, is the most common pattern of failure in these patients7.
Surgical approach
Oesophagectomy for cancer should aim at a radical (margin-negative) resection of the primary tumour and locoregional lymph nodes. It is recommended to resect a minimum number of 15 lymph nodes for adequate nodal staging but this can only be determined once the resection has been done8. Oesophageal cancer may advance via submucosal lymphatic channels and this should be carefully assessed at clinical staging and during surgery. This may influence how much oesophagus and/or stomach that needs to be resected in order to achieve a tumour-free margin16. For an optimal locoregional lymphadenectomy, a transthoracic approach is recommended as it has demonstrated a higher lymph node yield compared to the transhiatal (abdomen and neck) approach8,9,17. It remains unclear if a more extended resection also increases the chance of long term survival. The type of oesophageal resection is dictated by the location of tumour, location and risk of lymph node metastases, as well as the available choices for restoration of continuity. A gastric tube is preferred over the colon or jejunum given the accessibility and better postoperative functional outcomes.
The two main surgical approaches are transhiatal and transthoracic oesophagectomy. In the transhiatal technique, access to the distal thoracic oesophagus (up to the pulmonary veins) is achieved through the abdominal cavity. A cervicotomy is performed to transect the cervical oesophagus. The mid-thoracic oesophagus is bluntly dissected or removed with a vein stripper. Only peri-oesophageal lymph nodes around the distal oesophagus and in the abdomen can be removed whilst subcarinal and paratracheal nodal stations are left in situ. Transthoracic oesophagectomy involves opening of the chest (usually right chest) to dissect the oesophagus under vision and perform a mediastinal nodal dissection. The abdomen is entered for gastrolysis, creation of a gastric tube and nodal dissection. The two most common operations are the Ivor-Lewis technique, in which an intrathoracic oesophagogastric anastomosis is performed, and the McKeown technique, in which the oesophagus is transected via a cervicotomy and the anastomosis is created in the neck. Often the preference of the surgeon determines which technique to use. However, transhiatal oesophagectomy is associated with less pulmonary and cardiac complications and is thus mainly used for frail patients. The Ivor-Lewis oesophagectomy is associated with less swallowing and speech issues and less problems with gastric conduit emptying and gastroesophageal reflux, as compared to the McKeown technique. Moreover, the anastomotic leak rate is lower for Ivor Lewis (12.3%) compared to McKeown (34.1%), according to a recent randomized clinical trial from the ICAN research group, although in case of a leak, the clinical consequences and management of the leak might be more troublesome with an anastomosis located in the mediastinum18.
Recommended main surgical options and approaches according to tumour location are summarized in figure 1. Minimally invasive strategies -total laparoscopic and thoracoscopic, robotic assisted or hybrid approaches- may be associated with decreased postoperative mortality, shorter recovery times, and increased long-term survival, in comparison with the open approach8,19. Guidelines emphasize that oesophagectomy should always be performed in high-volume centers by experienced surgeons, where better postoperative short and long-term results have been demonstrated20.
How to select patients for a treatment?
As many patients diagnosed with oesophageal cancer are older than 70 years, patient’s fitness should be carefully assessed including any comorbidities, (history of) smoking and alcohol use. Although age and comorbidity are not clearly implemented in current treatment guidelines, they should also be taken into account when balancing risk and benefits before any therapeutic intervention21. It is important to judge if surgery is a realistic treatment option and if neoadjuvant chemo(radio)therapy treatment can be applied. For non-curative treatment options, symptoms that can be relieved by palliative interventions should be focused at. Current clinical practice guidelines recommend using the ECOG (Eastern Cooperative Oncology Group) scale and/or the Karfnofsky score (see table 2) in order to measure patient’s performance status (PS) and assess the medical fitness for any oncological treatment8-10. The discussion of treatment options with the patient should follow a shared decision-making model, where the patient’s wishes and preferences for treatment, and the impact of the disease and treatment on quality of life are all taken into consideration.
Table 2. Comparing the ECOG Performance Status and the Karnofsky Performance Status Scales
When the tumour is resectable, and if the patient is considered medically fit for surgery, further evaluations may be needed to assess patient’s fitness for surgery. Although there is no consensus, patients aged 75 years or older are generally recognized as elderly22,23. There is no absolute contraindication for surgery in elderly patients but clinical trials on which the guidelines are based often exclude elderly24. Although some suggest that octogenarians may not benefit from oesophagectomy22, others state that functional rather than chronological age is more important in decision-making. The consultation of a geriatrician can be very helpful21,22,24. Frailty should be routinely assessed in all patients, because a large proportion of older cancer patients are frail or pre-frail25. This leads to treatment-associated negative outcomes, including postoperative morbidity and mortality26. Assessment of frailty and QOL assessment seem to provide more prognostic information than performance status alone27,28, but there is still a lack of universally-accepted standard tools for evaluation.
Recently, on the basis of 10 preoperative variables (age, BMI, sex, ECOG performance status, history of myocardial infarction, connective tissue disease, peripheral vascular disease, liver disease, neoadjuvant treatment, and hospital volume), a risk prediction model of 90-day mortality after oesophagectomy for cancer was developed29. The model was created and validated based on a retrospective analysis of a total of 8403 patients from 39 institutions in 19 countries, using the International Esodata Study Group (IESG) database, the largest existing prospective, multicenter cohort reporting standardized postoperative outcomes. Although still independent validation of the risk score is needed, the model is easily accessible, provides an adjustment scoring system that permits comparison between practitioners and institutions, and provides an evidence-based schema for allocation of the most appropriate treatment on individual patient, so promisingly it could help in the decision-making process when surgery is being considered. Moreover, the cardiopulmonary fitness of the patient is predictive of postoperative major morbidity30. Involvement of the anesthesiologist in patient selection, preoperative and postoperative management has been associated with a lower rate of complications. Therefore, it is strongly recommended to have a specialized anesthesiologist as part of the MTB31. Some tools for the assessment of frailty, performance status and quality of life are shown in table 3. Figure 2 summarizes the evaluation of a patient with oesophageal cancer and the treatments available according to disease stage and patient characteristics.
Table 3. Some tools examples for patient’s fitness-for-surgery assessment
Figure 2. Simplified decision-making flowchart to be followed by the MTB when an oesophageal cancer is diagnosed. ADC: adenocarcinoma; SCC: squamous cell carcinoma; ENT: ear-nose-throat; dCRT: definitive chemoradiation.
New developments and future perspectives
New treatments for oesophageal cancer patients are mainly focused on improving life expectancy with better quality of life at lower costs. Immunotherapy aims to increase and restore the immune system’s ability to detect and destroy cancer cells by modifying and/or blocking co-stimulatory signals. Phase II and III trials suggest a survival benefit in oesophageal cancer patients treated with immune checkpoint inhibition32. Also targeted therapy, i.e. drugs to target specific genes and proteins that are involved in the growth and survival of cancer cells has been introduced. A selection of important drugs used in the treatment of oesophageal cancer are shown in table 4. At present, there are about 40 ongoing trials and 14 recently published trials with preliminary data. In the phase-III CheckMate-577 study, patients after neoadjuvant chemo-radiotherapy followed by oesophagectomy for stage II or III cancer were randomized to adjuvant nivolumab or placebo33. Disease-free survival was significantly longer among those who received nivolumab adjuvant therapy than among those who received placebo. Therefore, nivolumab is currently approved by the EMA (European Medicines Agency) and the FDA (Food and Drug Administration, USA) as adjuvant monotherapy for patients with completely resected oesophageal or OGJ cancer with residual pathologic disease who have received neoadjuvant chemo-radiotherapy. In addition, other immunomodulatory approaches such as peptide vaccines and tumour infiltrating lymphocytes (TILs) are currently under development.
Table 4. Biologic targeted agents and checkpoint inhibitors under assessment for oesophageal cancer.HER-2: Human Epidermal Growth Factor Receptor-2; PD-1: programmed cell death receptor 1; PD-L1: programmed cell death ligand 1; CTLA-4: cytotoxic T-lymphocyte-associated antigen 4; VEGF: vascular endothelial growth factor; EGFR: epidermal growth factor receptor.
Another new direction in the treatment of oesophageal cancer is active surveillance. After neoadjuvant chemo-radiotherapy, roughly half of the patients with squamous cell carcinoma and a quarter of those with adenocarcinoma have a pathological complete response (pCR) of the primary tumour before surgery. Thus, the necessity of standard oesophagectomy after neoadjuvant chemo-radiotherapy is now being called into question. The Surgery-As Needed-for Oesophageal Cancer (SANO) study group is currently evaluating active surveillance as a valid alternative to standard surgery in patients with a complete clinical response after neoadjuvant chemo-radiotherapy34-36, the first results are expected late 2023.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021 May;71(3):209-249.
He H, Chen N, Hou Y, Wang Z, Zhang Y, Zhang G, Fu J. Trends in the incidence and survival of patients with esophageal cancer: A SEER database analysis. Thorac Cancer. 2020 May;11(5):1121-1128.
Dubecz A, Gall I, Solymosi N, Schweigert M, Peters JH, Feith M, Stein HJ. Temporal trends in long-term survival and cure rates in esophageal cancer: a SEER database analysis. J Thorac Oncol. 2012 Feb;7(2):443-7.
SEER Training Modules, Anatomy of the Esophagus. U. S. National Institutes of Health, National Cancer Institute. 15 April 2022. <https://training.seer.cancer.gov/ugi/anatomy/esophagus.html>.
Rice TW, Kelsen DP, Blackstone EH, et al. Esophagus and esophagogastric junction. In: Amin MB, Edge SB, Greene FL, et al., editors. AJCC Cancer Staging Manual, 8th ed. New York: Springer, 2017:185-202.
Low DE, Kuppusamy MK, Alderson D, Cecconello I, Chang AC, Darling G, Davies A, D'Journo XB, Gisbertz SS, Griffin SM, Hardwick R, Hoelscher A, Hofstetter W, Jobe B, Kitagawa Y, Law S, Mariette C, Maynard N, Morse CR, Nafteux P, Pera M, Pramesh CS, Puig S, Reynolds JV, Schroeder W, Smithers M, Wijnhoven BPL. Benchmarking Complications Associated with Esophagectomy. Ann Surg. 2019 Feb;269(2):291-298.
Ng SP, Leong T. Indications for definitive chemoradiotherapy for oesophageal cancer. Ann Esophagus 2021;4:43.
National Comprehensive Cancer Network. Esophageal and Esophagogastric Junction Cancers (Version 2.2022) https://www.nccn.org/professionals/physician_gls/pdf/esophageal.pdf. Accessed March 27, 2022.
Lordick F, Mariette C, Haustermans K, Obermannová R, Arnold D; ESMO Guidelines Committee. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016 Sep;27(suppl 5):v50-v57.
Kitagawa Y, Uno T, Oyama T, Kato K, Kato H, Kawakubo H, Kawamura O, Kusano M, Kuwano H, Takeuchi H, Toh Y, Doki Y, Naomoto Y, Nemoto K, Booka E, Matsubara H, Miyazaki T, Muto M, Yanagisawa A, Yoshida M. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: part 1. Esophagus. 2019 Jan;16(1):1-24.
Wang H, Tang H, Fang Y, et al. Morbidity and Mortality of Patients Who Underwent Minimally Invasive Esophagectomy After Neoadjuvant Chemoradiotherapy vs Neoadjuvant Chemotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: A Randomized Clinical Trial. JAMA Surg. 2021;156(5):444–451.
Mungo B, Molena D, Stem M, Yang SC, Battafarano RJ, Brock MV, Lidor AO. Does neoadjuvant therapy for esophageal cancer increase postoperative morbidity or mortality? Dis Esophagus. 2015 Oct;28(7):644-51.
van der Wilk BJ, Eyck BM, Lagarde SM, van der Gaast A, Nuyttens JJME, Wijnhoven BPL, van Lanschot JJB. The optimal neoadjuvant treatment of locally advanced esophageal cancer. J Thorac Dis. 2019 Apr;11(Suppl 5):S621-S631.
Stahl M, Budach W. Definitive chemoradiotherapy. J Thorac Dis. 2017 Jul;9(Suppl 8):S792-S798.
Tougeron D, Di Fiore F, Thureau S, Berbera N, Iwanicki-Caron I, Hamidou H, Paillot B, Michel P. Safety and outcome of definitive chemoradiotherapy in elderly patients with oesophageal cancer. Br J Cancer. 2008 Nov 18;99(10):1586-92.
Worrell SG. Esophageal Cancer and Surgical Margins: When a Positive Is a Negative. Ann Surg Oncol. 2020 May;27(5):1316-1317.
Mertens AC, Kalff MC, Eshuis WJ, Van Gulik TM, Van Berge Henegouwen MI, Gisbertz SS; Dutch Upper GI Cancer Audit group. Transthoracic Versus Transhiatal Esophagectomy for Esophageal Cancer: A Nationwide Propensity Score-Matched Cohort Analysis. Ann Surg Oncol. 2021 Jan;28(1):175-183.
van Workum F, Verstegen MHP, Klarenbeek BR, Bouwense SAW, van Berge Henegouwen MI, Daams F, Gisbertz SS, Hannink G, Haveman JW, Heisterkamp J, Jansen W, Kouwenhoven EA, van Lanschot JJB, Nieuwenhuijzen GAP, van der Peet DL, Polat F, Ubels S, Wijnhoven BPL, Rovers MM, Rosman C; ICAN collaborative research group. Intrathoracic vs Cervical Anastomosis After Totally or Hybrid Minimally Invasive Esophagectomy for Esophageal Cancer: A Randomized Clinical Trial. JAMA Surg. 2021 Jul 1;156(7):601-610.
Gottlieb-Vedi E, Kauppila JH, Malietzis G, Nilsson M, Markar SR, Lagergren J. Long-term Survival in Esophageal Cancer After Minimally Invasive Compared to Open Esophagectomy: A Systematic Review and Meta-analysis. Ann Surg. 2019 Dec;270(6):1005-1017.
Brusselaers N, Mattsson F, Lagergren J. Hospital and surgeon volume in relation to long-term survival after oesophagectomy: systematic review and meta-analysis. Gut 2014; 63: 1393–1400.
Faiz Z, Plukker JTM. ASO Author Reflections: Implementation of Age and Co-morbidity in the Treatment Guideline of Patients with Esophageal Squamous Cell Carcinoma. Ann Surg Oncol. 2019 Dec;26(Suppl 3):585-586.
Motoyama S, Maeda E, Iijima K, Sato Y, Koizumi S, Wakita A, Nagaki Y, Fujita H, Yoneya T, Imai K, Terata K, Minamiya Y, Higashi T. Does Esophagectomy Provide a Survival Advantage to Patients Aged 80 Years or Older? Analyzing 5,066 Patients in the National Database of Hospital-Based Cancer Registries in Japan. Ann Surg. 2020 Dec 29.
Markar SR, Karthikesalingam A, Thrumurthy S, Ho A, Muallem G, Low DE. Systematic review and pooled analysis assessing the association between elderly age and outcome following surgical resection of esophageal malignancy. Dis Esophagus. 2013 Apr;26(3):250-62.
Hol JC, Heisterkamp J, Martijnse IS, Matthijsen RA, Langenhoff BS. Morbidity and mortality in elderly patients after minimally invasive esophagectomy. Ann Esophagus 2019;2:3.
Berg AS, Rostoft S. Frailty indicators in older cancer patients. Tidsskr Nor Laegeforen. 2019 Dec 3;139(18).
Rostoft S, Audisio RA. Recent advances in cancer surgery in older patients. F1000Research. 2017;6:1242.
Pearce J, Swinson D, Cairns D, Nair S, Baxter M, Petty R, Seymour M, Hall P, Velikova G; GO2 trial investigators. Frailty and treatment outcome in advanced gastro-oesophageal cancer: An exploratory analysis of the GO2 trial. J Geriatr Oncol. 2022 Apr;13(3):287-293.
Kidane B, Sulman J, Xu W, Kong Q, Wong R, Knox JJ, Darling GE. Pretreatment quality-of-life score is a better discriminator of oesophageal cancer survival than performance status. Eur J Cardiothorac Surg. 2017 Jan;51(1):148-154.
D'Journo XB, Boulate D, Fourdrain A, Loundou A, van Berge Henegouwen MI, Gisbertz SS, O'Neill JR, Hoelscher A, Piessen G, van Lanschot J, Wijnhoven B, Jobe B, Davies A, Schneider PM, Pera M, Nilsson M, Nafteux P, Kitagawa Y, Morse CR, Hofstetter W, Molena D, So JB, Immanuel A, Parsons SL, Larsen MH, Dolan JP, Wood SG, Maynard N, Smithers M, Puig S, Law S, Wong I, Kennedy A, KangNing W, Reynolds JV, Pramesh CS, Ferguson M, Darling G, Schröder W, Bludau M, Underwood T, van Hillegersberg R, Chang A, Cecconello I, Ribeiro U Jr, de Manzoni G, Rosati R, Kuppusamy M, Thomas PA, Low DE; International Esodata Study Group. Risk Prediction Model of 90-Day Mortality After Esophagectomy for Cancer. JAMA Surg. 2021 Sep 1;156(9):836-845.
Patel N, Powell AG, Wheat JR, Brown C, Appadurai IR, Davies RG, Bailey DM, Lewis WG. Cardiopulmonary fitness predicts postoperative major morbidity after esophagectomy for patients with cancer. Physiol Rep. 2019 Jul;7(14):e14174.
Deana C, Vetrugno L, Bignami E, Bassi F. Peri-operative approach to esophagectomy: a narrative review from the anesthesiological standpoint. J Thorac Dis. 2021 Oct;13(10):6037-6051.
Teixeira Farinha H, Digklia A, Schizas D, Demartines N, Schäfer M, Mantziari S. Immunotherapy for Esophageal Cancer: State-of-the Art in 2021. Cancers (Basel). 2022 Jan 22;14(3):554.
Kelly RJ, Ajani JA, Kuzdzal J, Zander T, Van Cutsem E, Piessen G, Mendez G, Feliciano J, Motoyama S, Lièvre A, Uronis H, Elimova E, Grootscholten C, Geboes K, Zafar S, Snow S, Ko AH, Feeney K, Schenker M, Kocon P, Zhang J, Zhu L, Lei M, Singh P, Kondo K, Cleary JM, Moehler M; CheckMate 577 Investigators. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N Engl J Med. 2021 Apr 1;384(13):1191-1203.
Noordman BJ, Spaander MCW, Valkema R, Wijnhoven BPL, van Berge Henegouwen MI, Shapiro J, Biermann K, van der Gaast A, van Hillegersberg R, Hulshof MCCM, Krishnadath KK, Lagarde SM, Nieuwenhuijzen GAP, Oostenbrug LE, Siersema PD, Schoon EJ, Sosef MN, Steyerberg EW, van Lanschot JJB; SANO study group. Detection of residual disease after neoadjuvant chemoradiotherapy for oesophageal cancer (preSANO): a prospective multicentre, diagnostic cohort study. Lancet Oncol. 2018 Jul;19(7):965-974.
Noordman BJ, Wijnhoven BPL, Lagarde SM, Boonstra JJ, Coene PPLO, Dekker JWT, Doukas M, van der Gaast A, Heisterkamp J, Kouwenhoven EA, Nieuwenhuijzen GAP, Pierie JEN, Rosman C, van Sandick JW, van der Sangen MJC, Sosef MN, Spaander MCW, Valkema R, van der Zaag ES, Steyerberg EW, van Lanschot JJB; SANO-study group. Neoadjuvant chemoradiotherapy plus surgery versus active surveillance for oesophageal cancer: a stepped-wedge cluster randomised trial. BMC Cancer. 2018 Feb 6;18(1):142.
Eyck BM, van der Wilk BJ, Noordman BJ, Wijnhoven BPL, Lagarde SM, Hartgrink HH, Coene PPLO, Dekker JWT, Doukas M, van der Gaast A, Heisterkamp J, Kouwenhoven EA, Nieuwenhuijzen GAP, Pierie JEN, Rosman C, van Sandick JW, van der Sangen MJC, Sosef MN, van der Zaag ES, Spaander MCW, Valkema R, Lingsma HF, Steyerberg EW, van Lanschot JJB; SANO-study group. Updated protocol of the SANO trial: a stepped-wedge cluster randomised trial comparing surgery with active surveillance after neoadjuvant chemoradiotherapy for oesophageal cancer. Trials. 2021 May 17;22(1):345.



.png)




