Equality, diversity and inclusion (EDI) within surgery is important.1 The recent Kennedy Review on Diversity and Inclusion, commissioned by the Royal College of Surgeons of England, made 16 recommendations to improve EDI in the surgical workforce.2 Cardiothoracic surgery in the UK lacks diversity, exemplified with only 13% of the consultant workforce being female, despite females accounting for 49% of UK doctors.3 One method of improving EDI in the specialty, is to focus on widening participation (WP) activities.
In the UK, WP activities and government policies aim to increase representation of lower socio-economic groups in higher education. Published schemes focus on peer-to-peer mentorship from medical to school students. The King’s College London scheme is a monthly seminar series offered to WP school students, publishing a 50% success rate of translation to successful application to medical school.4
We were unable to find a surgical specialty programme, and therefore The Society of Cardiothoracic Surgery (SCTS), set out to develop a WP initiative called INSINC Insight. The scheme was awarded the inaugural SCTS Equality, Diversity and Inclusion Award for 2024.
The project was designed and managed by the medical student committee, SCTS INSINC. It consisted of an online lecture series and face-to-face hospital placement, with Microsoft OneNote educational guide. Recognising the limited awareness of SCTS INSINC amongst school students, the lecture series was advertised predominantly via the Medical Schools' Council and national WP networks, allowing recruitment of students via their schools, and reinforcing promotion to this demographic. An online medical lecture platform, MedAll, was used to measure attendance and generate participant certificates. We did not refuse any attendee if they were already a medical student.
A customised, interactive study guide complemented all hospital placements, denoting information both specific to each hospital and general, practical information. It included descriptions of the multi-disciplinary team (MDT), FAQs, revision boards and suggestions for self-directed study and reflection. Students were expected to familiarise themselves with this prior to their placement, given the opportunity to ask any questions, and could refer to this throughout (Figure 1).
Figure 1
A generic timeline detailing the distribution of questionnaires, lecture series and hospital placements.
Impact of online lecture webinar series
Some 1292 attendances were recorded across 11 lectures, 736 in 2023 and 556 in 2024, with an average overall attendance of 117 students per lecture.
The demographic and background of students from the pre-lecture questionnaire was as shown in table 1.
Table 1
The demographic and background of participating students in the lecture series (respondents to the pre-lecture questionnaire).
|
Demographics
|
Percentage
|
|
Gender
|
78% female
|
|
Ethnic Minority
|
79%
|
|
Asian or Asian British
|
45%
|
|
Black, Black British, Caribbean or African
|
20%
|
|
Mixed or multiple ethnic groups
|
6%
|
|
Other ethnic minority not listed
|
8%
|
|
White
|
21%
|
|
Widening participation status
|
YES 42%
UNSURE 40%
17% NO
1% RATHER NOT SAY
|
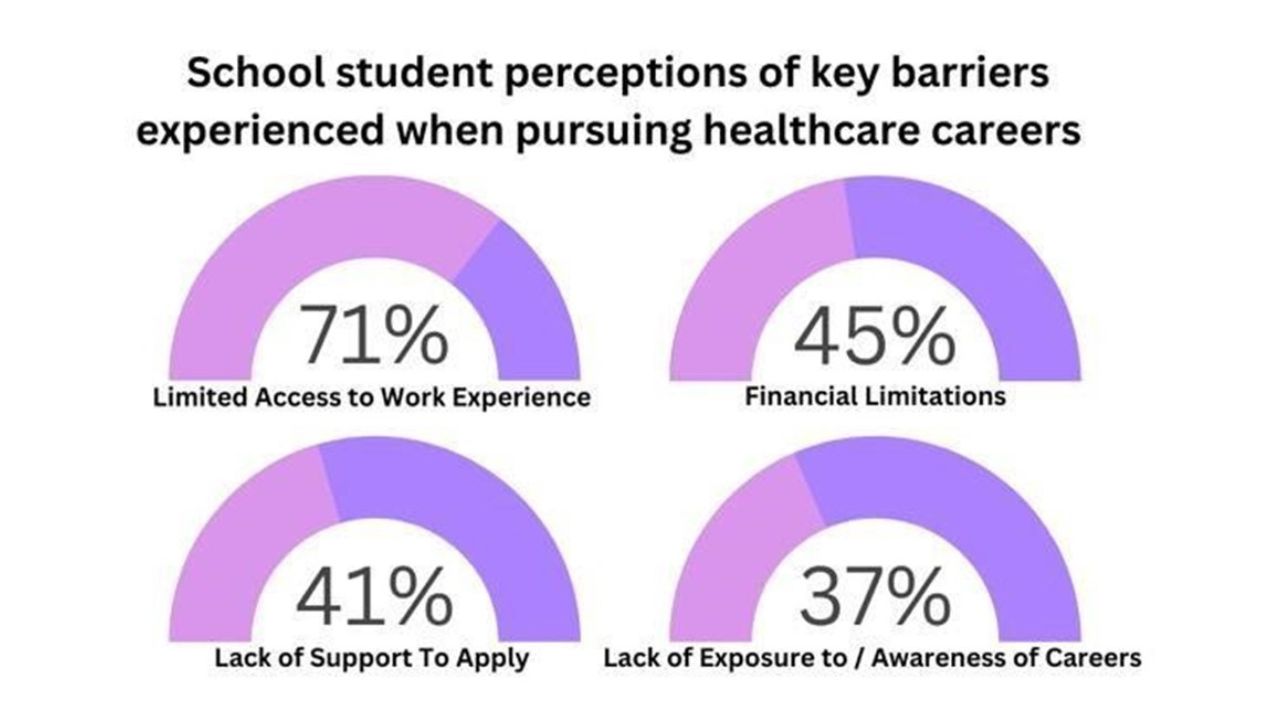
Students were asked what the key barriers were when trying to pursue a career in healthcare (Figure 2).
Figure 2
Summary of most common responses from school students when asked of barriers they'd experienced pursuing a healthcare career.
There was a total of 917 responses to the post-lecture questionnaire, 581 in 2023 and 336 in 2024 (average overall response rate 71%) (Figure 3).
Figure 3
A pictographic summary of the key take-home points from the results of pre-lecture and post-lecture questionnaires in 2023 and 2024.
Effect of clinical work experience placement
32 students participated in 5 centres over a two-year period. In 2023, 12 students were hosted in Bristol, Leicester and Leeds, and in 2024, 20 students were hosted in Bristol, Leicester, Edinburgh and Cambridge (Table 2).
Whilst it was not possible to entirely standardise the experience in each individual centre, all students had exposure to both clinical and non-clinical activities. Guidance of content for each placement was outlined to participating centres, prior to student attendance.
Table 2
The demographic of participating students in the placement (respondents to the pre-placement questionnaire).
|
Demographics
|
Percentage
|
|
Gender
|
50% female
|
|
Ethnic Minority
|
67%
|
|
Asian or Asian British
|
50%
|
|
Black, Black British, Carribean or African
|
8%
|
|
Mixed or multiple ethnic groups
|
5%
|
|
Other ethnic minority not listed
|
4%
|
|
White
|
33%
|
Students were also given the opportunity to provide written feedback for their placement, with key themes highlighting its focus on the wider MDT and other healthcare careers, whilst also providing a realistic insight into the hospital environment.
__
‘ I didn't realise there were so many other professions within medicine, which really made me realise the importance of the MDT.
’
‘ I gained an active insight into the multiple different careers that are available for me and realised that there are much more career options available in healthcare than I thought.
’
‘ It also provided reassurance that a career in healthcare can also be achieved through an alternative route such as pursuing another science degree.
’
‘ This was so interesting and engaging I am truly thankful to have been able to be part of this.
’
__
A year later, we followed-up on students who participated in 2023, ascertaining which career path they’d chosen and whether they felt this scheme had impacted their choice. Of the 11 students who agreed to follow-up, 4 provided updates. 2 obtained several offers to study medicine and 2 were unsuccessful in obtaining places, but plan to re-apply. In their feedback they wrote:
‘ This scheme showed me that it was the right path for me, and I learned many valuable skills.
’
‘ This scheme facilitated me to write up an EPQ, where I became fascinated with the mechanisms behind heart diseases
… and aided me in finding online courses..research..and books about CABG and ROSS [procedure].
’
‘ This scheme was incredibly useful during my applications and helped provide a more detailed insight into working as a clinician, in the NHS and other important job roles within the multidisciplinary teams.
’
__
Discussion
Compared to other WP schemes described in the literature, INSINC Insight is unique in two main areas, firstly, promotion of wider healthcare careers, such as perfusion, nursing and allied health professions and secondly, provision of supplementary educational resources prior to placements, which can be intimidating, unfamiliar environments.
We faced barriers in centre engagement, with many centres already running successful ‘work experience’ schemes, we were often asked why another was needed. We sought to provide assistance both in the specific selection of students from WP backgrounds, and, in supplying a specialty-approved educational tool, with material readily available and easily personalised to existing schemes.
We accept that the number of students impacted is inherently restricted, and that the success of the scheme, and experience offered, is somewhat dependent on enthusiasm of local centres. However, with a national society providing overarching support and, the development of a well-established framework for recruitment, the lecture series and educational tools, we feel this offers a degree of standardisation and reproducibility for other surgical specialties. In collaborating and rolling-out other national surgical specialty schemes, the potential for improving equality and diversity in surgery in the UK as a whole, is an opportunity we think should not be missed.
The scheme incurs minimal cost to run, with all speakers and consultant supervisors offering their time for free, however, with consideration of the entitlement to cost-neutral meals for WP students, SCTS charity funding enabled provision of lunch. With multi-centre success in this pilot, ultimately, we aspire for an annual, standardised scheme to be rolled out across all 34 cardiothoracic units within the UK and Ireland.
Direct translation into colleagues and subsequent improvement of diversity in specialty in the future is the most important metric of success for such schemes, consequently, we asked each participant consent to follow-up. In reporting these two-year outcomes, the intention is to highlight the importance of the scheme, however, in the future, we hope to publish the results of translation from opportunity into a career into specialty. We can report a 350% increase in the number of applicants for ST1 cardiothoracics, attributing partial responsibility to this scheme and our other student engagements initiatives. We will continue to monitor specialty applications and WP status in applicants and successful trainees, as a useful marker.
Number of applicants for Cardiothoracic Surgery ST1 NTN position
2018 – 90
2019 – 101
2020 – 129
2021 – 113
2022 – 137
2023 – 298
2024 - 408
Lessons learned to date include the importance of promoting the breadth of medicine by showcasing allied health professions and, ‘humanising’ surgery, by instilling confidence and empowering students through education, such as, ‘how to behave in the theatre environment’. It is crucial to create non-intimidating, welcoming environments to nurture students’ curiosity, therefore the choice in consultant supervisors is extremely important.
Key Suggestions
Following successful implementation of this scheme nationally, our key suggestions for those interested in offering a similar scheme are:
Engagement with local university WP officers and, where possible, local school networks to ensure broad reach of WP students.
Events should be free at the point of engagement for the student, and considerations of financial support for expenses, such as travel or meals, for face-to-face placements are beneficial.
Consideration should be given that some WP students may have time-restrictive responsibilities such as caring, therefore wherever feasible, all content should be accessible at the student’s preferred time. For example, recording events to be watched at a convenient time.
Appendix 1.
Criteria for inclusion into a widening participation scheme used for the INSINC Insight scheme
Lower socioeconomic status
Ethnic minority status
Students with disabilities
Students with caring responsibilities
Schools with low participation in higher education
(The scheme was presented to the Medical Schools' Council, resulting in contact being made with each universities widening participation officer to allow contact with local school headteachers to select students who met at least one of the above criteria.)
Acknowledgements
This scheme would not have been possible without the collaborative work of the INSINC Committees of 2021-2023 and 2023-2025. Recognition must also be given to the local hosts in each unit, including but not exclusive to; Mr Luke Roberts and Prof Hunaid Vohra (Bristol), Miss G Layton and Mr G Mariscalco (Leicester), Dr J Tariq (Leeds), Miss H Shamaz (Edinburgh), Miss M Hu and Mr J Ali (Cambridge).
References
1Harji D, Sarmah P, Gwyther B, Lyons MK, Boereboom CL, Siddiqi S, Arnott R, Harikrishnan A, Maxwell-Armstrong C, Cuming T; Association of Coloproctology of Great Britain and Ireland. Bridging that gap: a qualitative study of perceptions of equality, diversity and inclusivity in colorectal surgery in the UK and Ireland. BMJ Open. 2023 Jul 10;13(7):e069297. doi: 10.1136/bmjopen-2022-069297. PMID: 37429683; PMCID: PMC10335449.
2Royal College of Surgeons of England will put diversity at the heart of its strategy — Royal College of Surgeons (rcseng.ac.uk)
4Sanders G, Brett C, Paul N, Scott J. Creating Diversity in Tomorrow's Doctors: A Student Led, Widening Participation Outreach Programme. Adv Med Educ Pract. 2021 Jun 24;12:705712. doi: 10.2147/AMEP.S309178. PMID: 34211310; PMCID: PMC8240012.



.png)




