BJSOpen is a fully-online and open access journal & is proud to publish high-quality surgical research. This month, papers span surgical oncology, methdology, benign disease, and global surgery. The full table of contents is here.
We would also like to draw your attention to the EHS/AHS guidelines on primary hernias in rare locations or special circumstances.
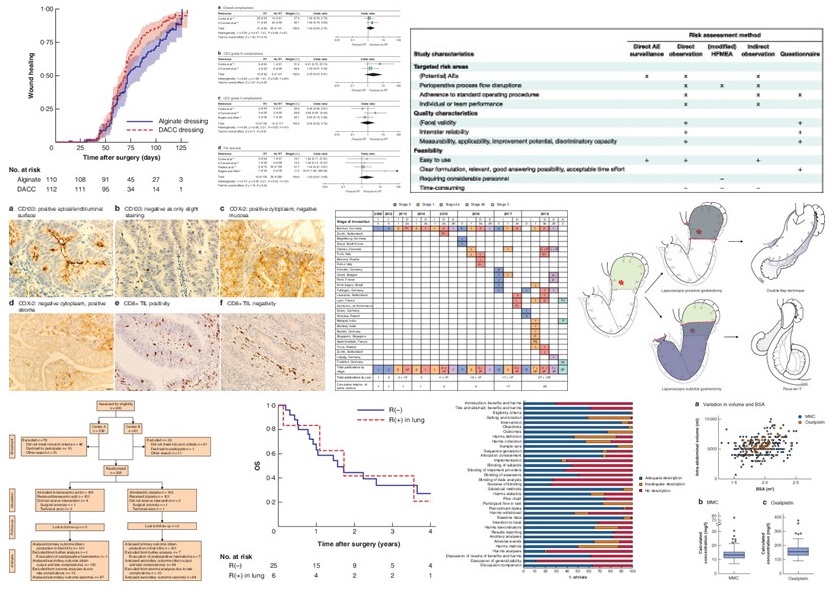
Some of the key images from this months papers
Methodology
Anyone submitting papers to a journal will be familiar with the role of checklists. These are intended to improve the quality of reporting of publications. This review has assessed how well benefits and harms of treatments are reported in surgical trials. It shows that the surgical community needs to do better; outcomes were poorly described, or presented in a manner where it was not possible to interpret effect sizes with any degree of precision.
Randomised trials
Whilst breast cancer surgery aims to conserve breast tissue, mastectomy is still an important tool for the breast surgeon. One of the problems seen here is with bleeding from this typically vascular area. This Norwegian trial randomised 208 patients to either topical tranexamic acid or topical saline to wound edges for haemostasis. There was reduced drain output in the TXA group. There was also a non-significant (but interesting) reduction in the rate of haematomas.
The pilonidal sinus is a sadly unloved condition. This is despite being a constant presence for the colorectal surgeon. This RCT compared alginate vs DACC (hydrophobic-type) dressings in wound healing after excision of pilonidal sinus. There was no difference in wound healing at 75 days on the per-protocol analysis. The trial needed 222 patients to complete to reach power calculations and managed to retain 200 patients. There might be other things to learn about trial management. This population is quite young and may pose problems with recruiting to trials
Surgical oncology
Other surgical oncology papers this month include a review of outcomes of immediate and delayed autologous breast reconstruction in post-mastectomy radiotherapy. This is a well conducted review and highlights the issues with the literature. On a related note, this patient survey on immediate breast reconstruction is interesting. It looks at some of the important socioeconomic factors that drive patient decision making around this treatment.
For the HPB surgeons, a cohort study shows the outcomes of resection for HCC with tumour thrombus extending into the IVC. In practice, this is a small group with advanced disease and this is shown by a 20 year case series. And not forgetting the oesophagogastric surgeons, we have a retrospective cohort study comparing laparoscopic proximal gastrectomy with double-flap technique versus laparoscopic subtotal gastrectomy for proximal early gastric cancer. This study was intended to assess the impact on nutrition between these two approaches. No difference in these outcomes were seen.
Advanced cancer
This is a growing field, and this growth is reflected in the many submissions we receive on this topic.Two of the big questions are on the prediction of development of peritoneal disease, and the role of chemotherapy dosing in HIPEC.
A large cohort study from the Danish Colorectal Database has tried to answer the first of these questions. Rates of metastatic peritoneal disease were low, but factors such as advanced tumour or node stage were associated with early presentations, whereas R1 resection was associated with recurrence at 3 years.
The second question was addressed by the PRODIGE 7 trial, which suggested cytoreductive surgery was key in treatment of peritoneal disease. This is reflected in a cohort study of ‘real world’ experience from the Netherlands. This has compared intraperitoneal chemotherapy outcomes based on agents used and adjusted for body surface area. It doesn’t seem to disagree with PRODIGE 7…
On a related note, the introduction of new technology demands robust assessment. For surgeons this typically follows the IDEAL framework. This review has looked at reports on the development of Pressurized intraperitoneal aerosol chemotherapy (PIPAC), which is based on laparoscopy to deliver intraperitoneal chemotherapy for peritoneal metastases. We now know that we are following the rules with this technology. However, progress is slow and we need bigger definitive studies to understand efficacy.
Global surgery
There are two papers on global surgery this month. One highlights the challenges related to deployment of electrosurgical and laparoscopic kit in LMICS. This shows that equipment is available, but surgeons still had problems using or maintaining it. The second paper shows that traumatic brain injury is common in Uganda, with a male preponderance. The mortality rate in this group is 33%. The authors suggest this may be influenced by limited access to CT and ICP monitoring.
Summary
These are just some of the papers published in this issue of BJSOpen. We welcome direct submissions to the journal. If you think your work would fit in here, please have a look at the instructions for authors page.





.png)




