A hypothesis paper on alternating population quarantine instead of lockdowns: a surgeon’s approach to the problem.
The Covid-19 pandemic is spreading quickly, threatening healthcare systems and the world economy. Test and tracing methods used efficiently in Asian countries are not feasible in countries with scarce test capacities. Current lockdown strategies are insufficient as not everyone can be quarantined for 2 weeks at the same time. An alternative strategy to extensive lockdown – namely an alternating home quarantine of half the population for 2 weeks at a time – is described in this post. This may be an efficient way to stop the spreading of the disease, buying time to establish test routines and a vaccine. At the same time it may prevent the economy and healthcare systems from collapsing.
As the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is newly identified, the actual case fatality rate (CFR) and susceptibility in the population are uncertain. During the Chinese outbreak the CFR was calculated to be 2.9% in the Hubei province compared to 0.4% outside Hubei (overall 2.8%) . In Italy it is at the moment 8.5% . The actual CFR is probably closer to 1% with optimal treatment capacities and early and complete detection. No natural immunity against the SARS-CoV-2 has been shown. Post exposure immunity after sub clinic infection is however probable, which would explain why the Chinese outbreaks outside Wuhan were less intense. Neither a vaccine nor approved treatment are currently available, although there are ongoing trials with several drugs both for treatment and prophylaxis.
Both South Korea and Singapore are conducting widespread testing of symptomatic patients combined with short-term lockdowns and tracing of close contacts to infected individuals. This strategy seems to have been very successful. Also China, where the virus originated, appears to have stopped the outbreak with combination of complete lockdown in hotspots, intensive testing and tracing, as well as restrictions in people’s mobility combined with partial lockdowns in other regions.
The rest of the world faces the challenge of widespread virus dissemination, which makes conventional containment measures as well as intensive test and tracing methods infeasible. Frankly, one doesn’t know where to look. In Italy, the European epicentre of the Covid-19 outbreak, a national lockdown was imposed the 9th of March. Several countries have introduced similar interventions with the aim “to flatten the curve”. The idea is to postpone and lower the peak of the epidemic curve to enable healthcare systems to cope, particularly with the high demand for mechanical ventilation. Another aspect of postponing instead of stopping the pandemic is the hope for so called “herd immunity” which will help to prevent later outbreaks.
All above-mentioned community interventions come at a very high cost. The world economy is starting to halt. As the current measures will need to be in place for a very long time, they may hinder sufficient supply of urgently needed equipment. Furthermore, it is uncertain whether the imposed actions are even close to slowing the pandemic sufficiently. The disease is highly contagious (R0 has been estimated between 2.4 and 3 in the Hubei Province and between 2.3 and 14.8 at the start of the Diamond Princess cruise ship outbreak) and even severe currently used community interventions will not entirely stop community transmission. Data from Italy for March 23rd show that the number of patients was still rising on average 14% the 10 preceding days; even in the region of Lombardy (first lockdowns February 27th) this figure was still 11% (down from 26% between Feb 23rd – Mar 3rd) although the number of new cases is finally declining. The Italian healthcare system is on the verge of collapse (Figure 1).
Figure 1: Newly diagnosed infections, active Covid-19 patients and Covid-19 patients in ICU in Italy, February and March 2020. The Intensive care unit (ICU) demand per million inhabitants raises proportional with the total number of patients with an ongoing Covid-19 infection. At the end of the period there are approximately 0.2% of the Lombardian population reported as Covid-19 positive creating a demand for 120 ICU beds per million Inhabitants. Even if the number of reported cases represents only 5% of the actual number it is clear that no healthcare system of the world can cope with a full-blown epidemic. (Data: Italian Ministry of health)
Currently, approximately 50,000 Italians are reported to have an ongoing Covid-19 infection. Even if the correct number was 20 fold (ascertainment in Wuhan was previously estimated to 5% (95%CI, 3.6–7.4)) that would be < 2% of the Italian population. One can only but imagine the consequences of 40% being infected. Currently, other European countries are struggling to prepare for the coming pandemic and consequently little aid is offered to Italy. The situation in the US is also currently escalating.
Hypothesis: A coordinated alternating nation- or region-wide quarantine of the whole population is an efficient way to stop the Covid-19 pandemic, with less impact on economies and on everyday life than the currently imposed partial lockdowns.
The idea is to divide the whole population in two groups (A and B) for a period of eight weeks. Both groups will stay in alternating home quarantine for two weeks at a time (quarantine length recommended by the WHO for Covid-19) while the other group attends to daily life. All symptomatic individuals during quarantine are either tested or need to remain in quarantine with their households. Positive tested individuals and their household members remain in home isolation until negative test result. Individuals in home-quarantine at the start of the first period are allocated to group A.
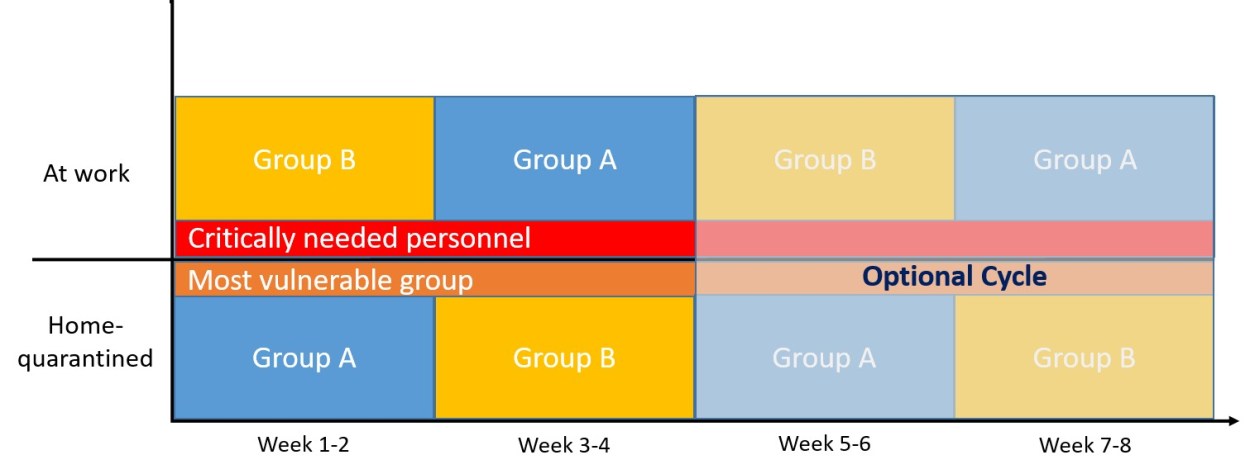
During this four-week period, other interventions should continue (cough and hand hygiene, social distancing, no public meetings, shut-down of cinema/theatres). Patients at risk should preferably be isolated for the whole period and some critical personnel might need to work the whole period (Figure2). The cycle may need to be repeated at the end of week 4 if there are many newly diagnosed patients in group A after the quarantine.
Figure 2: Schematic illustration of alternating quarantine. Preferably, the group of critically needed personnel should be as small as possible and avoid all contact with those practicing home quarantine. For personnel in regular contact with Covid-19 patients there should be a low threshold for testing. As reinfections are unlikely, healed personnel can work the whole period. Crossovers between from Group A to B are possible, for example if there is an urgent shortage of personnel or in case of emergency admissions, crossover from B to A is undesirable. Group A should preferably be a bit larger than group B in order to account for crossovers due to quarantines in Group B. To get a quick control of the situation in hotspots, Group A may be much larger than group B. Current restrictions like closed stores, cinemas, public meeting points, should be maintained at least for the first 4 weeks. If there are many new infections in group A at the end of week 4, the cycle needs to be repeated.
There are five prerequisites for this intervention to be effective:
It is essential that all members of one household are in the same group.
The group in home quarantine needs to stay at home and either buy all supplies for 2 weeks before the start of the period, or be supplied by the community (i.e. by the group that is not quarantined); this is to prevent new infections. Only few exceptions should be made (for example chronically ill or acutely unwell patients in need of hospital treatment and patients receiving home nursing or staying in institutions).
There should be as little contact as possible (preferably no contact) between the groups when switching quarantine periods. Non-avoidable contacts need to be traceable.
The start of the two periods needs to be coordinated for large areas, preferably whole countries, or country unions (for example the whole European Community).
At the end of each period, public areas and workspaces need to be disinfected thoroughly due to the long-lasting stability of the virus on surfaces.
There are different ways to allocate the population to the groups – community wise, according to where people work (for example a whole factory may pause for 2 weeks as long as household members of employees are allocated to the same group), by postal code or house number. The optimal way may differ between countries and communities. Group A may be larger than group B in order to get a quick control of the situation, especially in Hotspots. The whole 4-week circle needs to be followed by an active surveillance with intensive testing. A detailed plan by domestic health authorities for workers in critical positions who need to work throughout the whole period can minimize the chance of “contamination” of Group A and B after the home quarantine periods (for example home delivery of food to those working with Covid-19 patients). Figure 3 shows a very simplified model of the effect of social distancing and lockdowns compared to alternating quarantine.
Figure 3: Simplified model of the effect of moderate community interventions, partial lockdowns and alternating population quarantine to prevent the spread of Covid-19.Figure 3a & 3b: Number of infected individuals at the end of a four week period with two different scenarios of community interventions if 2 out of 500 were infected at the start: 3a Local lockdowns, travel restrictions and other interventions, daily increase of infected individuals by 10% assumed (current situation in Italy, at the beginning of the outbreak the daily increase was >20%). 3b Rigid lockdown as effectuated in Italy the 9th of March. This intervention is here estimated to reduce the daily increase to 7%; the effect is expected to be visible on the epidemic curves the coming days and may be larger.Figure 3c – 3f: The effect of an alternating home quarantine (gridlines) assuming a daily increase of infected individuals of 10% in the not quarantined population. In a perfect situation with all patients becoming symptomatic, all would be detected and isolated at the end of week 4. However, the model is neither accounting for not quarantined asymptomatic patients living in other household than symptomatic patients, nor for insufficient test capacities at the end of the period being in the way for testing also individuals with little symptoms, which is why the circle needs to be repeated if there are many new infections in Group A at the end of week 4.
The main strength of alternating population quarantine is that the risk of community acquired Covid-19 infection is reduced to a minimum already after week 2. Furthermore, this concept would enable countries to stop the pandemic quickly locally. The impact on economy would be minimalized as several businesses can run for a short period of time with half the workforce. Temporary working hour adjustments or reduction in activity may compensate for the loss of work force.
The concept has some drawbacks. It requires either complete compliance by the population or effective control mechanisms with law enforcement. However, when confronted with the alternative of a never-ending partial shutdown combined with a probable major recession or that of staying at home for a limited time, the choice should be easy and politicians should be able to motivate the majority of the public to stay at home for two weeks at a time.
Another aspect is the susceptibility of the population for a new outbreak due to lack of immunity. However, the cycle of home quarantine can be repeated if necessary until sufficient test capacities, vaccines or treatments are available which is still preferable to a never-ending partial lockdown. Asymptomatic Covid-19 positive patients may prevent the success of this method. The proportion of asymptomatic patients has been estimated to be 18% during the Diamond Princess cruise ship outbreak.
It is likely that asymptomatic individuals will often be in close relation to symptomatic ones. A double cycle could allow us to identify almost all; it is however even more difficult to conduct. Experience from Asian countries shows that quarantine and isolation measures do work and that it is sufficient to test those who are symptomatic in order to find asymptomatic transmitters. When new clusters are detected, the method may even be repeated in affected areas. Many adaptions of this method are possible. Advanced epidemiological models and increasing knowledge about the disease may help to optimize it. The main principle however remains: to reliably separate the infected population from the non-infected in space and time.
At the moment, many countries are expanding ICU capacities. In my own hospital, this is possibly to a six-fold of normal capacity, and this may not even be enough. Furthermore, the current pandemic already prevents elective patients from receiving care. In addition, the current situation causes major damage to the world economy. Although the number of newly infected patients in Italy has been falling the last two days, there may be a quick raise again once restrictions are lifted. We should therefore do whatever we can to stop the pandemic rather than postpone its peak. This is not only to protect the old and vulnerable, but also to save our healthcare systems and our societies from collapsing and to avoid a new era of Great Depression. To quote one principle of damage control surgery: “the treatment of bleeding is to stop the bleeding”. The current approach is similar to treating a bleeding patient with transfusions and a simple bandage to slow the bleeding.
Ethical aspects
One might argue that it is unethical to expose group B for transmission longer than group A. However, the risk of infection for group B will be reduced considerably compared to what it is now already in when group A is quarantined. Furthermore, the exposure for Group B could be minimized by increasing the Size of group A. Two weeks of strict home quarantine may also increase the risk of home violence; this is however not much different from lockdowns.
Conclusion
With the current knowledge about Covid-19, the current strategy of delaying the pandemic seems to hazardous. The present hypothesis of alternating home quarantine can only be tested by governments of countries or provinces, but time is precious.
Acknowledgements
I would like to thank my colleagues and family for critical discussions. I would also like to thank Sheraz Yaqub and Ørjan Olsvik for a critical review of the paper. Further, I thank my Italian colleagues Michela Monteleone and Dario Tartaglia for inside information from the epicenter of the European outbreak.
Disclosures
None other than a close bond to Italy, #tuttoandrabene! Funding: none.



.png)




