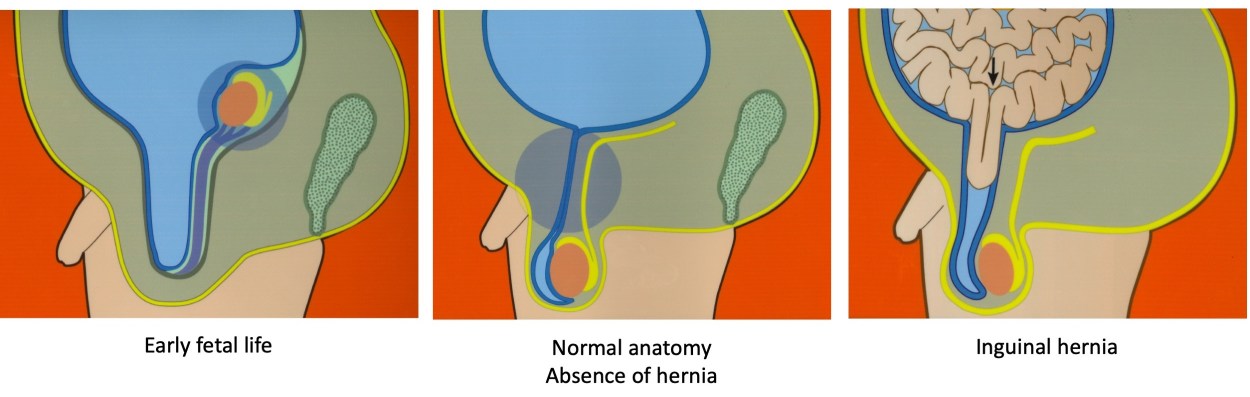
Are women who have inguinal hernias more likely to have a child with an inguinal hernia? Have you ever wondered why a child may develop an inguinal hernia? Inguinal hernias affect about 4% of children1,2, but the reasons why are very unclear. An inguinal hernia occurs when intestinal tissues push through a weak spot in the abdominal wall. Most children with inguinal hernias are thought to have developed this disorder while still in their mother’s womb1,3. Yet there has been little attention to the possibility that the characteristics of mothers could predict which children will develop inguinal hernias while growing up.
We studied whether women who were previously diagnosed or treated for an inguinal hernia were more likely to have a child with an inguinal hernia. To test our research question, we analyzed the health status of 795,590 children from the province of Quebec, Canada4. We collected information from their mothers including her age, pregnancy complications, diseases she may have had in the past, and whether she was ever treated for an inguinal hernia. We closely followed her child over time to find out if the child was ever hospitalized for an inguinal hernia between birth and 13 years of age. We used regression methods to determine how characteristics of the mothers were associated with the chance of having an inguinal hernia in the child, and made sure that we controlled for confounders that could lead to incorrect measurements.
Our findings were very enlightening. We confirmed that mothers with a history of inguinal hernia were more likely to have a child who develops an inguinal hernia. But we found that the risk was higher for daughters than sons. Girls whose mothers had an inguinal hernia were 5 times more likely to themselves have an inguinal hernia. Additionally, mothers with connective tissue disorders such as rheumatoid arthritis or lupus were more likely to have sons with inguinal hernias. The figure illustrates just how strong some of the associations were.
These results suggest that the characteristics of a mother may affect a child’s chance of having an inguinal hernia. The likelihood of having an inguinal hernia also depends on if the child is a girl or a boy. Some of this difference may be because the development of inguinal hernias in boys is not the same as in girls. But it is also possible that there is a genetically sex-linked component. Finally, the relationship between maternal connective tissue diseases and the risk of inguinal hernia in boys suggests that connective tissue architecture may be involved as well.
Although more research is needed to confirm these findings, doctors and patients should be aware that children with abdominal symptoms who have a mother with a history of an inguinal hernia or connective tissue disorder may themselves be more likely to have an inguinal hernia. For more information, we invite you to read our study that was recently published in British Journal of Surgery4.
References
Azarow K, Cusick R. Pediatric Surgery [Internet]. The Surgical clinics of North America, Vol. 92. 2012. Available from: http://www.sciencedirect.com/science/article/pii/S0039 610912000680 [accessed 11 February 2021]
Lao OB, Fitzgibbons RJ, Cusick RA. Pediatric inguinal hernias, hydroceles, and undescended testicles. Surgical Clinics of North America 2012; 92: 487–504.
Kapur P, Caty MG, Glick PL. Pediatric hernias and hydroceles. Pediatric Clinics of North America 1998; 45: 773–789.
Auger P, Del Giorgio F, Le-Nguyen A, Bilodeau-Bertrand M, Piché N. Pediatric hernias and hydroceles. British Journal of Surgery 2021.



.png)



