Competing interests: The authors declare no competing interests.
Funding: No funding was provided for this study.
Previous presentations: The findings of this study were presented as a poster at the Society for Surgery of the Alimentary Tract 60th Annual Meeting on the 21st May 2019.
The reach of tweets: #SoMe4Surgery – #SSAT19 poster by @rebgross#SMSS19pic.twitter.com/Y1CiJf24GZ' Julio Mayol (@juliomayol) June 22, 2019
Introduction
It has long been the tradition to publish the Proceedings of surgical conferences 1. Over the last 15 years, the way surgeons interact has transformed extensively due to the advent of social media, with much of the conversation moving online 2-3. The covid-19 pandemic acted to accelerate this transition 4. The microblogging platform Twitter provides a vast library of information and allows real-time communication and dissemination of information, grouped along themes via a “hashtag” (metadata tag) 5-8. Twitter use is increasing among surgeons, researchers, healthcare professionals, and patients.
Organised conversations on Twitter, so-called “tweetchats”, are a forum through which experts, trainees, and patients from around the globe can communicate and discuss topics of shared interest via a hashtag and moderated by a host 5,7,9. Tweetchats allow real-time back and forth conversation, similar to face-to-face interactions10. These conversations are a treasure-trove of ideas that can provide great insight into the most cutting-edge trends in surgical practice 7,11-13.
On 28th July 2018, a social media initiative was created by Julio Mayol via his Twitter handle (@juliomayol), to focus on specific surgical interests, connected via the hashtag #SoMe4Surgery (Social Media For Surgery) 14. The aim was to bolster a more inclusive, multidisciplinary surgical community. Since the inception of #SoMe4Surgery, a number of tweetchats were planned and undertaken using the hashtag. In November 2018, a tweetchat was held with the subject of surgical technology. This theme was chosen as surgical technology is rapidly evolving in many directions, under multiple influences 15, and the authors felt it was a key time to take stock in where we are and where we are going. The aim of this study was to identify the main themes of the chat on surgical technology and to estimate the potential reach of the tweets.
Methods
Ethics
No ethical approval was required for this retrospective study as it did not interfere with any patient or human data beyond measuring internet activity among Twitter users using publicly available tweets.
Sampling and data extraction
A retrospective analysis was performed of the tweetchat that was led by two surgeons with 941 (@rebgross) and 24,539 (@juliomayol) followers on November 23rd 2018, with ten predefined questions. The #SoMe4Surgery ecosystem was the primary target of the conversation. Ten tweets containing questions for the audience were posted in a 60-minute period (9:00 pm – 10:00 pm Madrid time).
Analytics
Data analytics and visualization were carried out using two different online tools. Twitonomy is available at http://www.twitonomy.com, and provides advanced network analytics of tweets, hashtags and tweetchats, under subscription. Twitonomy analytics were performed by author JM on November 29th 2018, of tweets posted between November 22nd 2018 at 8:15 pm and November 29th 2018 at 8:17 pm using the two hashtags, “#some4surgery” and “#surgicaltechnology”. Potential reach was defined as the total aggregate number of followers of the people who mentioned both keywords in their tweets. Potential reach may be overestimated as Twitonomy may make assumptions to estimate impressions and/or audience, and geolcations are sometimes misclassified; therefore NodeXL analytics were also examined by author GM. NodeXL is a spreadsheet template that allows the creation of visual network graphs (Social Media Research Foundation; California, USA; https://www.smrfoundation.org/nodexl/). Using NodeXL, the extracts for 23rd November 2018 were extracted and mapped as described elsewhere 16.
The tweets from the tweetchat were manually reviewed on Twitter by author RG by searching for the terms [#SoMe4Surgery since:2018-11-23 until:2018-11-30] on 18th June 2019 to identify the themes of the chat for content analysis. Replies to the questions posted by the moderators were also reviewed to avoid missing tweets that did not include the hashtag. The handles (usernames) and profiles of the users were manually reviewed.
Results
Analytics
Twitonomy analytics revealed that, between 22nd November 2018 at 8:15 pm and 29th November 2018 at 8:17 pm, there were 348 tweets and retweets including the two hashtags posted by 60 users (40 men, 13 women, 7 unknown) from 50 geolocations in 5 continents. From the biographical information available in their Twitter profiles, specialties included general surgery (5), HPB/transplant (4), plastics/cosmetic (2), vascular (4), ophthalmology (1), hernia (1), colorectal (5), cardiovascular (1), endocrine/bariatric (1), spinal (1), global (1), trainees (1), associations (1), and non-medical (5). Conflicts of interest of individuals participating in the tweetchat included working for private health tech companies (4), criminal defence lawyer (1), and running the tweetchat (2).
From Twitonomy, the potential reach was 1,883,455 accounts. A tweetmap of the users of both #SoMe4Surgery and #SurgicalTechnology hashtags can be found in Fig. 1.
Fig. 1. Tweetmap of the users of both #SoMe4Surgery and #SurgicalTechnology hashtags
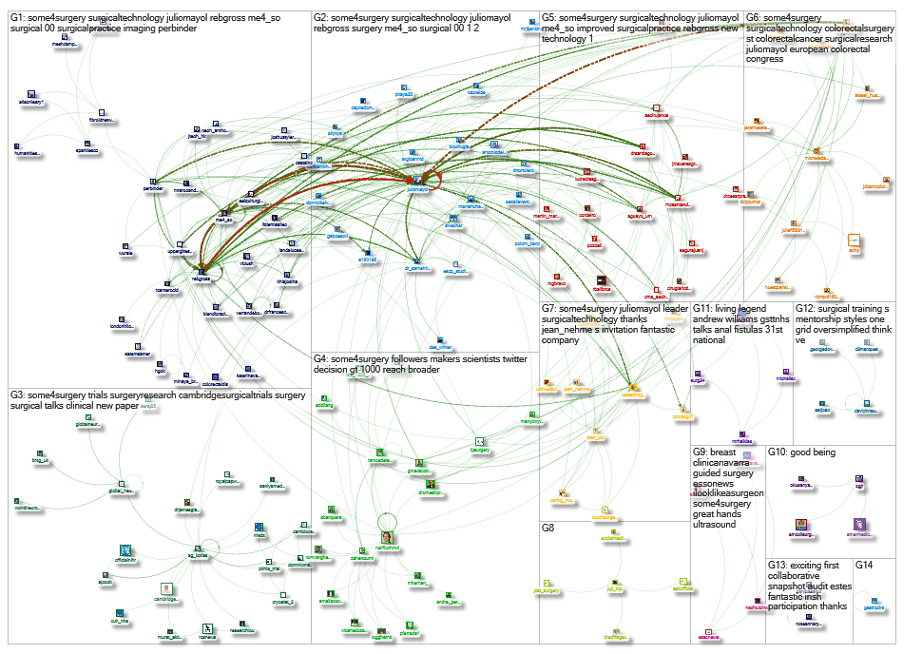
NodeXL data revealed, over the 1-day, 2-hour, 48-minute period from Thursday, 22nd November 2018 at 19:15 UTC to Friday, 23rd November 2018 at 22:04 UTC, there was a network of 39 Twitter users whose recent tweets contained both #SoMe4Surgery and #surgicaltechnology hashtags (Fig. 2), or who were replied to or mentioned in those tweets. There were 39 vertices, 71 unique edges, 303 edges with duplicates, 374 total edges, and 22 self-loops. Reciprocated vertex pair ratio was 0.19, and reciprocated edge ratio was 0.32. In a connected component, there were 39 maximum vertices and 374 maximum edges.
Fig. 2. NodeXL graph of twitter users whose tweets or mentions contained the hashtags #SoMe4Surgery and #SurgicalTechnology. The graph is directed. The graph’s vertices were grouped by cluster using the Clauset-Newman-Moore cluster algorithm. The graph was laid out using the Harel-Koren Fast Multiscale layout algorithm.
Over the 21-hour, 40-minute period from Friday, 23rd November 2018 at 00:18 UTC to Friday, 23rd November 2018 at 21:59 UTC, there was a network of 152 Twitter users whose recent tweets contained the #SoMe4Surgery hashtag (Fig. 3), or who were replied to or mentioned in those tweets. There were 152 vertices, 329 unique edges, 546 edges with duplicates, 875 total edges, and 44 self-loops. Reciprocated vertex pair ratio was 0.13, and reciprocated edge ratio was 0.22. In a connected component, there were 128 maximum vertices and 848 maximum edges.
Fig. 3. NodeXL graph of twitter users whose tweets or mentions contained the hashtag #SoMe4Surgery. The graph is directed. The graph’s vertices were grouped by cluster using the Clauset-Newman-Moore cluster algorithm. The graph was laid out using the Harel-Koren Fast Multiscale layout algorithm.
From Twitonomy, the ten most influential users (8 men, 1 woman, 1 unknown) had a median number of followers of 16,648 (range 747-344,648). The ten most engaged users (4 men, 3 women, 3 unknown) posted a median number of 27 tweets (range 11-346). The top hashtags were #SoMe4Surgery, #surgicaltechnology, #surgicalpractice, #AI and #SSI.
Current technological improvements to surgical practice
In a poll asking which surgical technology has most significantly improved surgical practice (Question 4), preoperative imaging received the most votes (53% out of 288 votes), with intraoperative imaging receiving 10% of the votes (Fig. 4). @WarrenRozen stated that preoperative imaging is certainly of benefit, while intraoperative imaging has not yet demonstrated this effect despite having great potential. @MrRJEgan stated that preoperative imaging reported by specialists can improve quality and outcomes. @perbinder highlighted that this was particularly important in vascular surgery, where preoperative Duplex and CT angiography are widely used. @SJ_Chapman suggested that in colorectal surgery, medical imaging in general had revolutionised patient care before, during and after surgery, for example with the use of post-processing CT colonography, PET-CT, and MR. @EUrologyReg agreed, stating that the now widespread availability of CT scans has had a huge impact on surgical decision-making.
Fig. 4. Screenshot of Question 4 of the tweetchat. Poll: “Which surgical technology has more significantly improved your surgical practice?”
Energy delivery systems received 33% of the votes. @DrSantiagoOrtiz explained that technologies such as laser, phacoemulsification, and vitrectomy had revolutionised his field of ophthalmology. @MrRJEgan stated that the main benefit of energy devices lies in efficiency and reduced operating times.
Biomaterials received the fewest votes (4%) and were considered more likely to be of benefit in the future (@WarrenRozen), although @DrSantiagoOrtiz thought that they were becoming very relevant in ophthalmology with the use of intraocular lenses.
@A160186 reported that endoscopy and endoluminal surgery have also changed the face of surgery, and that interventional radiology has radically impacted the management of surgical conditions, pointing out that it is a non-surgical technology, and that saving the patient from having an operation should be considered an achievement in itself. @DrSantiagoOrtiz agreed that non-surgical technology will likely have the highest impact in surgical practice.
In a poll asking which surgical technology is most frequently used for intraoperative bleeding (Question 7), 82% of the 102 votes were for energy delivery devices, 10% for fibrin sealants, and 2% for thrombin gels (Fig. 5). @YorkLawLondon stated that intraoperative bleeding can be problematic in fibroid surgery, and that pharmacological therapy, such as preoperative hormone suppressants and intraoperative vasopressin, is frequently used to counter this.
Fig. 5. Screenshot of Question 7 of the tweetchat. Poll: “What surgical technology do you most frequently use for intraoperative bleeding?”
In a poll asking about the use of surgical technology to reduce the rates of surgical site infection in surgical practice (Question 5), 40% voted “yes” (of 78 respondents), 22% voted “sometimes”, and 31% voted “no” (Fig. 6). @DrSantiagoOrtiz expressed surprise by the high proportion answering “no”, stating that the use of such technology is widespread in ophthalmology.
Fig. 6. Screenshot of Question 5 of the tweetchat. Poll: “Do you use any surgical technology to reduce the SSI rates in your surgical practice?”
Future innovations in surgical technology to improve patient safety
A wide range of technological innovations were proposed to improve patient safety in future surgical practice. These included energy devices, advances in anaesthesia, pharmacology, information technology services and data management, radiology and nuclear medicine, and advances in medical allied medical specialities such as gastroenterology, clinical genetics, and medical oncology.
An area in which many Twitter users were interested was navigation-guided surgery, particularly with respect to finding the right planes and avoiding at-risk structures (@dr_samehhany81). @A160186 described a “surgical GPS or an intraoperative Siri/Alexa” to guide surgeons through tough terrain. @polom_karol took this further, adding a preoperative diagnostic tool overlay and the help of artificial intelligence to assist in surgical decision making.
“It would be great if during a lap cholecystectomy [you] could just go ‘Siri [please] tell me if this is the cystic duct’ (hoping she’d have the right answer).” (@A160186)
@Eric_Vibert and @jamestoml1 both highlighted the importance of the OR Black BoxTM in changing the relationship between surgery and human error, which has a significant impact on patient safety. @schnitzb suggested that direct loop feedbacking would lead to a reduction in human error.
The most commonly mentioned technological advance was laparoscopic and robotic surgery. @CelestinoGutirr argued that robotic surgery improves the technical precision of surgery; @alessiominuzzo countered that as it has been introduced as an “instrument” and its indications have altered, its use should be considered “off label surgery”, or should only be in the context of research. It was compared to laparoscopy, with @RNCsantander and @anhanssen suggesting that the outlook for robotics was similar to that of laparoscopy in its early days, and @DrSantiagoOrtiz stating that the evidence has shown laparoscopy to improve patient safety, while the jury is still out for robotics. Overall, the consensus was that, in the future, the evidence would reveal robotic surgery to be beneficial to patient safety.
In a poll asking how robotic surgery will evolve in the future (Question 2), 42% of respondents (134 votes) predicted that robots would be smaller (Fig. 7). Only 11% of respondents thought that robotic surgery would be phased out. @tuttlejebetsy argued that the “the case reimbursement is too low for sustainability and widespread adoption”, suggesting that robotic surgery only has a future as long as it can demonstrate a sustainable, cost-effective return on investment.
Fig. 7. Screenshot of Question 2 of the tweetchat. Poll: “How will robotic surgery evolve in the future?”
@RNCsantander questioned how we can improve the learning curve and training in robotic surgery to generalize its use. The high cost of the technology was felt to be a barrier to its accessibility (@A160186, @RNCsantander, @rcanterocid). @rebgross suggested the use of simulation training, and @A160186 suggested that robotics should be included in training or fellowship programmes, arguing that one must have seen it to practise, and subsequently teach, the technique. @JoshuaTylerMD stated that skill monitoring and improved mentorship via online platforms were essential in improving training.
Three-dimensional printing for surgical practice
In a poll, 51% of 164 individuals voted to say that three-dimensional (3D) printing might be useful for surgical practice (Question 6), while 35% said it will have a big impact, and 7% voted for “it’s a fad” (Fig. 8).
Fig. 8. Screenshot of Question 6 of the tweetchat. Poll: “What is your opinion on 3D printing for surgical practice?”
Participants of the tweetchat had found 3D printing to be useful in colorectal (@dr_samehhany81) 17, orthopaedic and maxillofacial (@rcanterocid), and vascular surgery (@TMCAvascular).
@GaneshPuttu and @JasamineCB both stated that 3D printing has been useful in complex cases or with complex anatomy, to assist in visualisation for pre-operative planning, as well as an education tool for trainees and patients, with @MMakgasa suggesting they be used in the consent process. @TMCAvascular called 3D printing fundamental for case planning, posting “before” and “after” images of a ruptured cannulation site pseudo-aneurysm treated with an atrial septal device via brachial approach with intravascular ultrasound and intracardiac echography with the aid of 3D printing.
For case planning it's fundamental. Here is a patient with a ruptured cannulation site pseudo aneurysm treated with an atrial septal device via brachial approach with IVUS, ICE and ECHO. Before and after 3-D printed pics. @jmills1955@benstarnesmd @LumsdenHMDHVC pic.twitter.com/SkF6iCbSj4' Vascular Surgery and Endovascular Therapy (@5280vascular) November 26, 2018
@LumsdenHMDHVC stated that his centre had moved away from 3D printing for training purposes, for which they used virtual simulation, but that its use was better indicated in case planning and device printing. @jmills1955 thought that the ability of 3D printing to allow the creation of patient and anatomic-specific devices would lead to it having a significant impact. @VerranDeborah echoed its use for implants and extended this to the biofabrication of tissue, suggesting that it may pave the way for the printing of organs in 10-20 years.
Artificial intelligence and its impact on surgical practice
Overall, the consensus was that artificial intelligence (AI) had the potential to have a significant impact on surgical practice. @juliomayol suggested that AI will change the way decisions are made and outcomes are monitored. @dr_samehhany81 and @Dr_A_Sturiale countered that AI would aid and complement the work of humans, but will never replace them.
In particular, it was thought that AI would have the largest impact in medical specialties in which imaging plays a crucial role in diagnosis (@DrSantiagoOrtiz). It was also felt that AI may result in a lower workload and administrative burden, with more time left to devote to direct patient care (@schnitzb). @polom_karol had a dramatic view of AI, stating: “AI will change all”, and that it was “the biggest revolution since [the] early beginning of surgery.” @hgok went so far as to suggest that in only 10 years, appendicectomies and cholecystectomies would be performed by AI-controlled robotic platforms, but that in hernia surgery this would take more time to develop.
@A160186 felt that one of the biggest benefits of AI would be found in patient safety, by creating “safety checkpoints” in clinical decision making, leading to the standardisation of diagnostics and procedures. She added that it was not clear whether AI would ever be autonomous; @YorkLawLondon and @DSoybel suggested this would mean it would only be as good as the data entered, and, for example in diagnostics, a diagnosis could be missed. @DSoybel further posed the critical question of who would control the data and algorithms. @YorkLawLondon added that any outsourcing could lead to companies exploiting or restricting data access and profiting from it; @DSoybel answered: “If neither data nor algorithms are proprietary there would be chaos. If both are proprietary there would be monopoly and potential for gaming. If one is and the other is not, there will be competition.”
“I’m sure surgeons prefer artificial intelligence over lack of intelligence.” @A160186
The patient’s perspective
There were some very insightful answers given when patients were asked which surgical technology they most valued. They can be found here. The most common theme was that the surgeon was valued above the technology.
Ethical issues in the development of new surgical technology
The issue of data ownership again arose when discussing the ethical issues surrounding the development of new surgical technology (@polom_karol).
The evaluation of risks and benefits was frequently mentioned (@CelestinoGutirr, @RNCsantander). Other issues included the dangers of optimism bias (@rebgross), as not all innovations are successful or result in improved patient care, and publication bias (@SJ_Chapman), leading to research waste 18. @SJ_Chapman also stated that it is ethically essential to determine not only if biotechnology results in patient benefit, but also the mechanics of why it works and has benefit, and that this would require well-designed qualitative work and patient and public involvement to facilitate the future development of the technology. @DrJamesGlasbey raised the issues of learning curves, proctorship, and early outcomes reporting. @schnitzb added the problems of rushing a product into market based on inadequate data. Finally, @coezycoe suggested that value and cost would have an impact on patient access to new surgical technology.
“[We] need to avoid ‘try it, bin it’ attitudes when evaluating surgical [biotechnology].” @SJ_Chapman
Discussion
Principle findings
The tweetchat reached a global audience across different surgical specialties, as well as attracting engagement from patients.
The form of surgical technology currently found to be the most useful among the tweetchat participants was preoperative imaging. Energy delivery systems were the most commonly used technology to assist with intraoperative bleeding. Most participants employed surgical technology to reduce the rates of surgical site infection. Exciting avenues for future innovation included navigation-guided surgery, increased use of the OR Black BoxTM, and developments in laparoscopic and robotic surgery. The use of 3D printing and AI were both considered to increase in the coming years, with potential advances in automation. There were numerous important ethical issues to consider when developing new surgical technology. Finally, the consensus among patients was that, while advances in surgical technology were welcome, they were not as important or valued as the surgeon who employs them.
Limitations of analytics
It should be noted that Twitter polls are unvalidated and subjected to selection bias, and one person may also control multiple accounts. Although some users provide information about their areas of expertise in their Twitter bios, this is unregulated, and they may not include conflicts of interest. There is therefore the risk of non-expert or uncited opinions being included in the synthesis. This caveat must be emphasised when sharing such data.
Some data may be confounded by “incidental retweeting”, whereby if a tweeter uses two hashtags together, it is not always possible to determine from which hashtag the retweet results. Third party social media tools tend to overestimate impressions and audience. Although Twitter Analytics may provide a more accurate measure of impressions, this is not possible to collect from a tweetchat in which multiple Twitter accounts are engaged. Finally, collecting such data is subject to the Hawthorne effect, where changes in behaviour may be affected by the act of observation 19.
To validate the findings, further research could incorporate validated methods of qualitative research, such as thematic analysis.
Conclusions
Social media may be used to disseminate information within a vast surgical ecosystem, engaging surgeons with a strong social media presence. The use of a standardised hashtag in a tweetchat allows information to reach a high volume of global Twitter users in the surgical community in a short space of time. Tweetchats between a diverse group of surgeons, allied health professionals, and the general public, can be a goldmine for determining the direction of future surgical innovations.
Acknowledgements
The authors are grateful to the #SoMe4Surgery community for continued support.
References
Dukes CE. Discussion on major surgery in carcinoma of the rectum with or without colostomy, excluding the anal canal and including the rectosigmoid: general results of surgical treatment. Proc R Soc Med. 1957;50(12):1031-1035.Mayol J, Dziakova J. Value of social media in advancing surgical research. Br J Surg Volume 104, Issue 13, December 2017, Pages 1753–1755, https://doi.org/10.1002/bjs.10767
Grajales FJ, Sheps S, Ho K, Novak-Lauscher H, Eysenbach G. Social media: a review and tutorial of applications in medicine and health care. J Med Internet Res. 2014;16(2):e13. doi:10.2196/jmir.2912.
Keller DS, Grossman RC, Winter DC. Choosing the new normal for surgical education using alternative platforms. Surgery (Oxf). 2020 Oct;38(10):617-622. doi: 10.1016/j.mpsur.2020.07.017. Epub 2020 Aug 30.
Elmously A, Salemi A, Guy TS. The Anatomy of a Tweet: Social Media in Surgical Practice. Seminars in Thoracic and Cardiovascular Surgery. 2018;30(3):251-255. doi:10.1053/j.semtcvs.2018.02.008.
Xu WW, Chiu I-H, Chen Y, Mukherjee T. Twitter hashtags for health: applying network and content analyses to understand the health knowledge sharing in a Twitter-based community of practice. Qual Quant. 2014;49(4):1361-1380. doi:10.1007/s11135-014-0051-6.
Mackenzie G, Grossman R, Mayol J. Beyond the hashtag: describing and understanding the full impact of the #BJSConnect tweet chat May 2019, BJS Open, 2020;, zraa019, https://doi.org/10.1093/bjsopen/zraa019
Brady R R W, Chapman S J, Atallah S, Chand M, Mayol J, Lacy A M, Wexner S D, #colorectalsurgery. Br J Surg. Volume 104, Issue 11, October 2017, Pages 1470–1476, https://doi.org/10.1002/bjs.10615
Hawkins CM, Hillman BJ, Carlos RC, Rawson JV, Haines R, Duszak R Jr. The Impact of Social Media on Readership of a Peer-Reviewed Medical Journal. Journal of the American College of Radiology. 2014;11(11):1038-1043.
Topf JM, Sparks MA, Phelan PJ, et al. The Evolution of the Journal Club: From Osler to Twitter. American Journal of Kidney Diseases. 2017;69(6):827-836. doi:10.1053/j.ajkd.2016.12.012.
Grossman RC. This month on Twitter. Br J Surg. 2019;106(7):814-814. doi:10.1002/bjs.11255.
Litchman ML. Diabetes Online Community User Perceptions of Successful Aging With Diabetes: Analysis of a #DSMA Tweet Chat. JMIR Aging 2018;1(1):e10176 https://agingjmirorg/2018/1/e10176/. 2018;1(1):e10176.
Bolderston A, Watson J, Woznitza N, et al. Twitter journal clubs and continuing professional development: An analysis of a #MedRadJClub tweet chat. Radiography. 2018;24(1):3-8. doi:10.1016/j.radi.2017.09.005.
Grossman RC, Mackenzie DG, Keller DS, Dames N, Grewal P, Maldonado AA et al. #SoMe4Surgery: from inception to impact. BMJ Innov 2020;6:72–82 http://dx.doi.org/10.1136/bmjinnov-2019-000356
Jayne DG. Relationship between surgeons and industry, Br J Surg, Volume 106, Issue 8, July 2019, Pages 965–967, https://doi.org/10.1002/bjs.11241
Mackenzie G, Murray AD, Oliver CW. Virtual attendance at an international physical activity meeting using Twitter: how can data visualisation provide a presence? Br J Sports Med. 2018 Mar;52(6):351-352.
Emile SH, Wexner SD. Systematic review of the applications of three‐dimensional printing in colorectal surgery. Colorectal Dis. 2018;2017:ArticleID4574. doi:10.1111/codi.14480.
Chapman SJ, Aldaffaa M, Downey CL, Jayne DG. Research waste in surgical randomized controlled trials. Br J Surg. 2019 Oct;106(11):1464-1471. doi: 10.1002/bjs.11266. Epub 2019 Aug 8.
Fry DE. The Hawthorne Effect Revisited. Diseases of the Colon & Rectum. 2018;61(1):6-7. doi:10.1097/DCR.0000000000000928.



.png)




