Have you ever worried if you or a loved one has bowel cancer? Bleeding from the rectum, changing bowel habits, unexplained weight loss, abdominal pain and bloating are symptoms many have been conditioned to associate with bowel cancer, warranting a visit to the doctors. However, studies have demonstrated that presence of these symptoms are poor predictors of colorectal cancer diagnosis.(1)
Currently, when these symptoms are raised with your doctor, it is very likely that the next step would be a colonoscopy or colonography. This involves clearing your bowel with bowel preparation laxatives for the test and discomfort of having a medical instrument inserted into one’s back passage. These colonic investigations also carry small but significant procedural risks.
The faecal immunochemical test, or FIT, is a simple and non-invasive test for patients who present to their doctors with symptoms concerning for bowel cancer. It is stool test that can reliably detect minute amounts of human blood in faeces that is not always visible to the naked eye. Most bowel cancers bleed to varying degrees into the colon and mix with faeces. FIT has been widely used in bowel cancer screening programmes but surprisingly it is only with COVID constraining access to healthcare that interest to expand its clinical use for patients with bowel cancer symptoms has taken hold.
We hypothesised that the FIT test could measure the amount of blood in faeces of patients presenting with concerning symptoms and categorise them into different colorectal cancer risk groups to help doctors determine the need for and urgency of recommending further invasive colonic investigation.
At the end of August 2021, we looked at over 9600 relevant academic publications on this topic, selected 15 high quality studies that were best designed to answer the question and combined their results for further analysis.
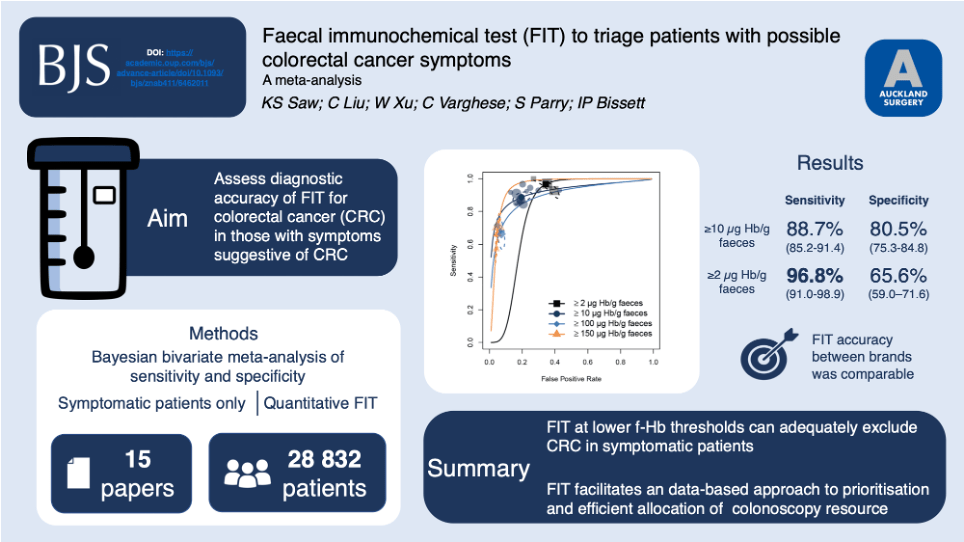
Our analysis showed that at the lowest possible detectable faecal blood by FIT (≥2 microgram Hb/g faeces), a positive FIT test would detect approximately 96 out of 100 colorectal cancers. In two of the largest studies conducted in the UK (2, 3), up to 63% of patients who under current standards would undergo an invasive colonic investigation because of reported symptoms, would be able to avoid one.
When settings are adjusted to be in line with current National Institute for Health and Care Excellence (NICE) recommendations (≥10 microgram Hb/g faeces), a positive FIT test would pick up approximately 88 out of 100 colorectal cancers. If one has a negative FIT test at this setting, it is estimated that approximately only 1 in 243 patients undergoing invasive colonic investigation would have a cancer detected, meaning by contemporary practices, 242 patients would undertake the risk of a colonoscopy despite not having bowel cancer. (2,3)
Conversely, if FIT detects higher levels of blood in faeces (such as at ≥100 or ≥150 microgram Hb/g faeces), approximately 1 in 3 patients will have bowel cancer diagnosed.
For patients with symptoms, these results indicate that when very low levels of blood are detected in stool by FIT, the chances of having bowel cancer are adequately low, hence invasive investigation may be avoided. Conversely, if relatively higher levels of blood are indicated by FIT, the probability of an existing bowel cancer is very high and urgent colonic investigation would be ideal to detect and treat the cancer as soon as possible.
No test is perfect. The currently accepted gold standard, colonoscopy, is estimated to miss 5 in 100 cancers.(4) With the correct settings, our analysis suggests that FIT approximates this diagnostic accuracy while being non-invasive, accessible and cheap. While colonic imaging tests have an irreplaceable role in the diagnosis of bowel cancer, it may be more optimal for patients, clinicians, and health care systems to rationalise the use of colonoscopy and colonography to avoid delays in diagnosis and treatment for those who are deemed to be at highest risk of bowel cancer.
There are more intricacies related to this question and areas requiring further research, hence, for more information, we invite you to read our Open Access article that was recently published in BJS.
References
Vega P, Valentin F, Cubiella J. Colorectal cancer diagnosis: Pitfalls and opportunities. World J Gastrointest Oncol. 2015;7(12):422-433.
D’Souza N, Georgiou Delisle T, Chen M, Benton S, Abulafi M, Group NFS. Faecal immunochemical test is superior to symptoms in predicting pathology in patients with suspected colorectal cancer symptoms referred on a 2WW pathway: a diagnostic accuracy study. Gut. 2021;70(6):1130-1138.
Turvill JL, Turnock D, Cottingham D, Haritakis M, Jeffery L, Girdwood A, et al. The Fast Track FIT study: Diagnostic accuracy of faecal immunochemical test for haemoglobin in patients with suspected colorectal cancer. British Journal of General Practice. 2021;71(709):E643-E651.4. Pickhardt PJ, Hassan C, Halligan S, Marmo R. Colorectal cancer: CT colonography and colonoscopy for detection–systematic review and meta-analysis. Radiology. 2011;259(2):393-405.





.png)




