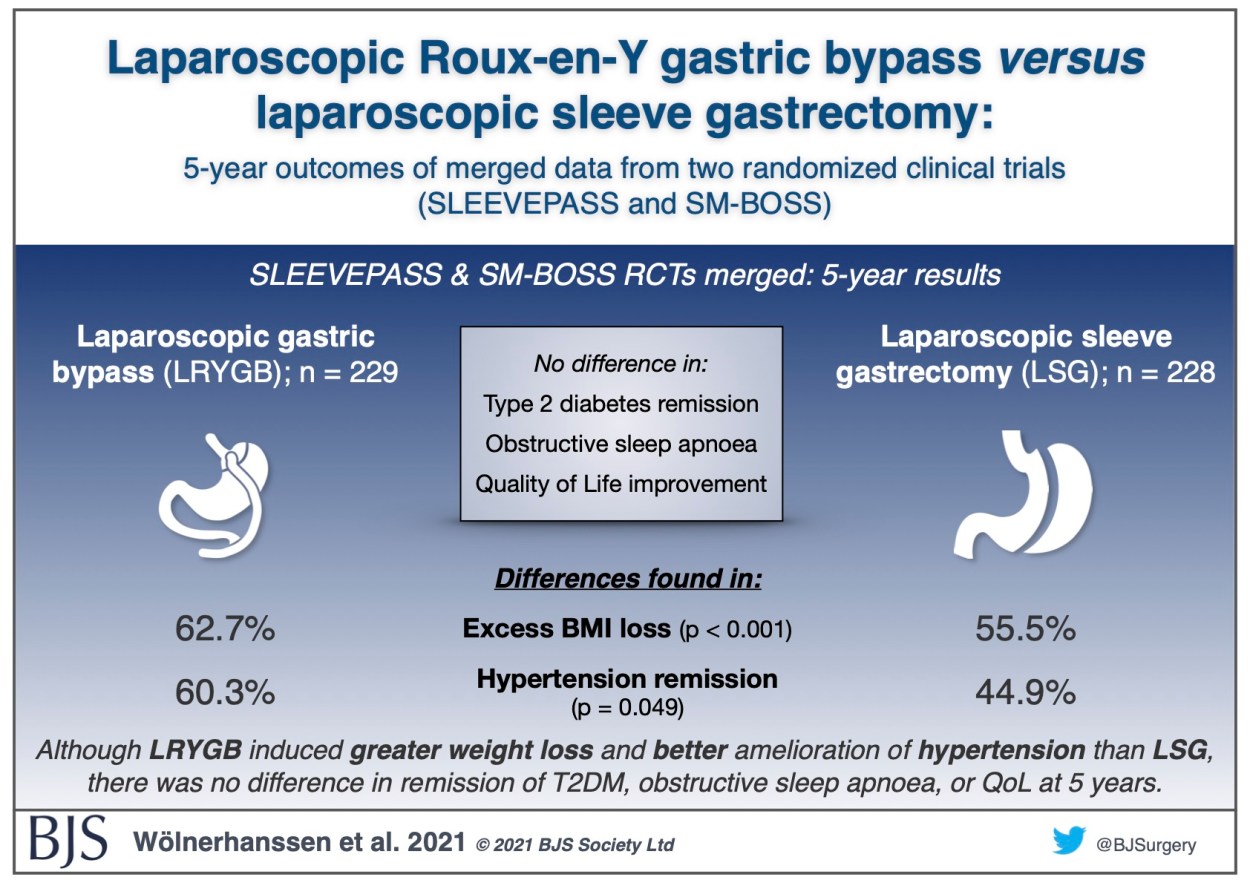
Laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy: 5-year outcomes of merged data from two randomized clinical trials (SLEEVEPASS and SM-BOSS)
Recently published as open access in BJS, the 5-year results of the merged Finnish SLEEVEPASS and Swiss SM-BOSS randomised controlled trials comparing laparoscopic sleeve gastrectomy with laparoscopic Roux-en-Y gastric bypass shows that Roux-en-Y led to greater weight loss and better control of hypertension than sleeve gastrectomy, with no difference in outcomes for type 2 diabetes, obstructive sleep apnoea, or quality of life. More details can be found in the paper.



.png)




