Keyhole surgery (laparoscopic appendicectomy) has been the mainstay of adult appendicitis treatment in Europe and the United States for the last several decades. In spite of this numerous trials have been ongoing exploring if there is a role for non-operative management of appendicitis with antibiotics. The APPAC and CODA trials both demonstrated that antibiotics were effective at treating simple appendicitis that was not perforated, gangrenous or associated with an abscess in the majority of patients.(1,2) However, it remained an underutilised treatment strategy.
This all changed during February and March of 2020, when the Sars-COV-2 virus (COVID-29) swept across much of the globe. Healthcare providers were forced to make contingency plans for hospitals that faced being overwhelmed by patients infected with COVID-19. Much of the anaesthetic workforce had been redeployed to intensive cares and there was uncertainty of the safety of general anaesthesia for patients with peri-operative COVID-19 and of the safety of the theatre teams exposed to virus aerosols during laparoscopy.(3,4) Non-operative management strategies were implemented recommended by surgical professional bodies across many surgical disciplines as a way of mitigating for these uncertainties.(5)
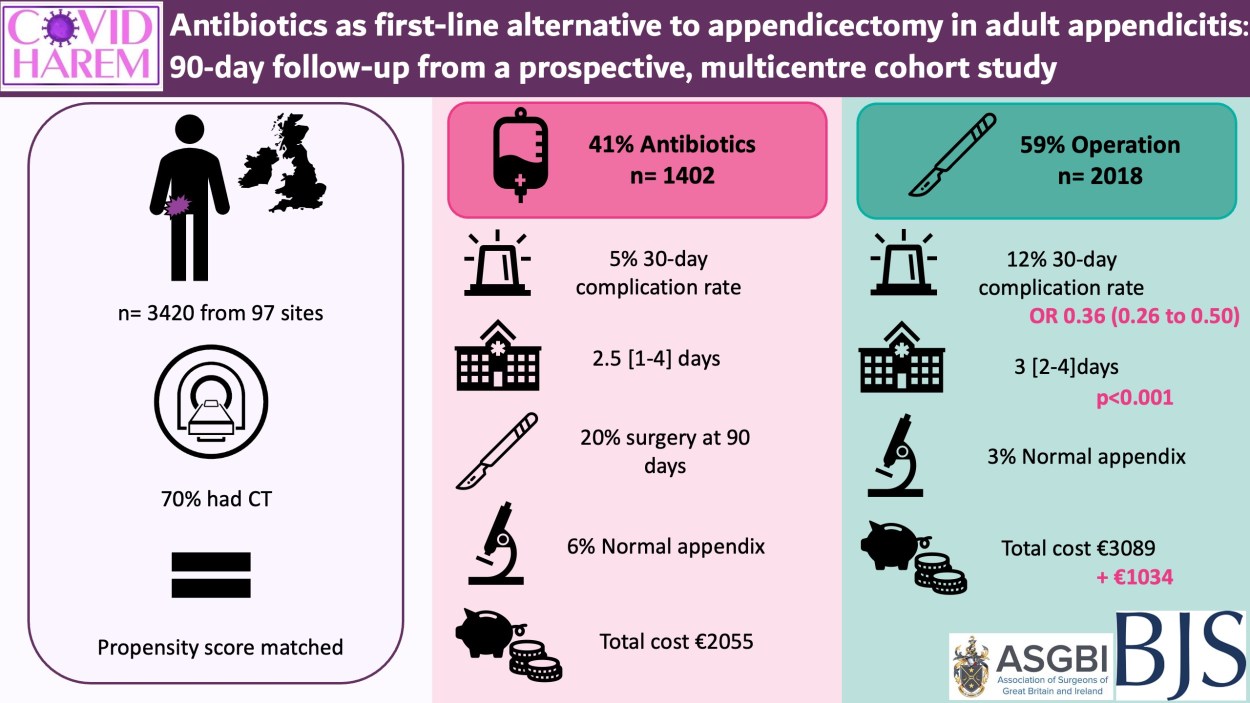
Our collaborative’s report, just published in BJS, represents the first time non-operative management of appendicitis has been implemented on a wide scale in the United Kingdom. We collected data on patients over the age of 18 presenting during the first wave of the COVID-19 pandemic presented with signs and symptoms suggestive of acute appendicitis, whether they were managed operatively and non-operatively. These patients were followed up for 90 days for length of hospital stay, complications, representation to hospital and appendicitis recurrence. Patients managed non-operatively were matched with similar patients managed operatively using propensity score matching, and their outcomes were compared.
Patients from 97 hospitals across the United Kingdom and Republic of Ireland were included in our study. Three thousand four hundred and twenty patients were included, of which 41% had initially been treated with antibiotics. When they were matched using propensity score matching with similar patients who had non-operative management, the group treated with antibiotics spent less time in hospital and had fewer complications than those who had an operative management. Non-operative management was successful in 80% of the patients managed in this way, with 20% going on to have an appendicectomy in the 90 days after their first attendance.
We also teamed up with a health economics team from the London School of Tropical Medicine to calculate the costs associated with each treatment method. We found that, even when accounting for the 20% of patients that had surgery within the 3 months of being treated with antibiotics, non-operative management was associated with a cost reduction of €1034 per patient compared to operative management.
This study proves that antibiotics are an effective management strategy for appendicitis and can be utilised on a large scale beyond trials for the first time ever. Patients may be keen to avoid surgery for a number of reasons and going forward surgeons should incorporate a discussion about the risks, benefits and uncertainties of non-operative management into conversations they have with patients about appendicitis management options. Our results have shown how reducing the number of operations we do for appendicitis can have benefits for the patient in terms of complications and days in the hospital away from work and home, but it may have wider benefits to the hospital and world. Not only is non-operative management cheaper for the hospital, but reducing the number of appendicectomies performed can free up theatre time so the most urgent surgical emergencies have less delay accessing theatre. All operations are associated with a significant amount of carbon emissions and single use plastic waste, but despite our best efforts to reduce the harm that surgery can cause to the environment the most effective strategy remains reducing the amount of unnecessary surgery performed.(6)
That is not to say that the study of non-operative management of appendicitis is over, there is still debate about the long-term efficacy of antibiotic management and concern that some cancers of the appendix may be missed by not removing the appendix at the first presentation, as well as questions about how acceptable patients find non-operative management. Our collaborative hopes to answer these questions and more in a one year follow up study and ongoing patient and public involvement work.
Conflicts of Interest
None to declare
Funding
No funding was received for this blog article
References
Salminen P, Tuominen R, Paajanen H, Rautio T, Nordström P, Aarnio M, et al. Five-year follow-up of antibiotic therapy for uncomplicated acute appendicitis in the APPAC randomized clinical trial. JAMA. 2018 Sep 25;320(12):1259–1265.
CODA Collaborative, Flum DR, Davidson GH, Monsell SE, Shapiro NL, Odom SR, et al. A Randomized Trial Comparing Antibiotics with Appendectomy for Appendicitis. N Engl J Med. 2020 Nov 12;383(20):1907-1919.
Nepogodiev D, Bhangu A, Glasbey JC, Li E, Omar OM, Simoes JF, et al. Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: an international cohort study. Lancet [Internet]. 2020 Jul 4 [cited 2020 Nov 5];396(10243):27–38. Available from: https://doi.org/10.1016/
SH E. Should we continue using laparoscopy amid the COVID-19 pandemic? Br J Surg [Internet]. 2020 Jul 1 [cited 2021 Sep 5];107(8):e240–1. Available from: https://pubmed.ncbi.nlm.nih.gov/32432344/
Hettiaratchy S, Deakin D. Guidance for surgeons working during the COVID-19 pandemic from the Surgical Royal Colleges of the United Kingdom and Ireland. Intercollegaite Royal Colleges of Surgery. London; 2020.
MacNeill AJ, Lillywhite R, Brown CJ. The impact of surgery on global climate: a carbon footprinting study of operating theatres in three health systems. Lancet Planetary Health [Internet]. 2017 Dec 1 [cited 2021 Sep 5];1(9):e381–8. Available from: http://www.thelancet.com/article/S2542519617301626/fulltext





.png)




