Normal View Dyslexic View
Insurance status may impact on survival from malignant cardiac tumours
13 July 2022
Guest Blog Vascular
Related articles

Plain English Summary: How the first COVID‐19 wave affected UK vascular services
The COVID-19 pandemic has impacted healthcare around the world. Patients who have vascular disease (problems with their arteries or veins), are at high-risk of having complications if they develop COVID-19. This is because patients with vascular disease usually have many medical problems. Some of them are also elderly and might be frail. We do not know how the COVID-19 pandemic might have affected the care of patients with vascular disease.
The COVER study is an international study trying to assess how the COVID-19 pandemic changed the medical care of patients with vascular disease. The first part of the COVER study was an internet survey. In this survey, doctors and healthcare professionals were asked questions (every week) about the care of vascular patients at their hospital. The results were published in this article.
The results showed that the COVID-19 pandemic had a major impact on vascular services worldwide. Most of the 249 hospitals taking part from 53 countries, reported big reductions in numbers of operations performed and the types of services they could offer to patients with vascular disease. Almost half of the hospitals stopped doing routine scans to detect artery problems and a third had to stop all clinics in the height of the pandemic. There were major changes in the resources available to treat blocked leg arteries. Most non-urgent operations, especially for vein problems, were cancelled.
Guest blog: Cerebral microbleeds following thoracic endovascular aortic repair
W. Eilenberg a,b**, M. Bechstein d**, P. Charbonneauc, F. Rohlffs a, A. Eleshra a, G. Panuccio a, J. Bhangu b, J. Fiehler d, R. Greenhalgh e, S. Haulon c, T. Kölbel a*
a German Aortic Center, Department of Vascular Medicine, University Heart & Vascular Center, University Hospital Hamburg-Eppendorf, Hamburg, Germany
b Department of General Surgery, Division of Vascular Surgery, Medical University of Vienna, Vienna, Austria
c Centre de l’Aorte, Hôpital Marie Lannelongue, Groupe hospitalier Paris Saint Joseph, Université Paris Saclay, France
d Department of Diagnostic and Interventional Neuroradiology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
e Vascular Surgical Research Group, Imperial College, London, UK.
** both authors contributed equally
E-mail:
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
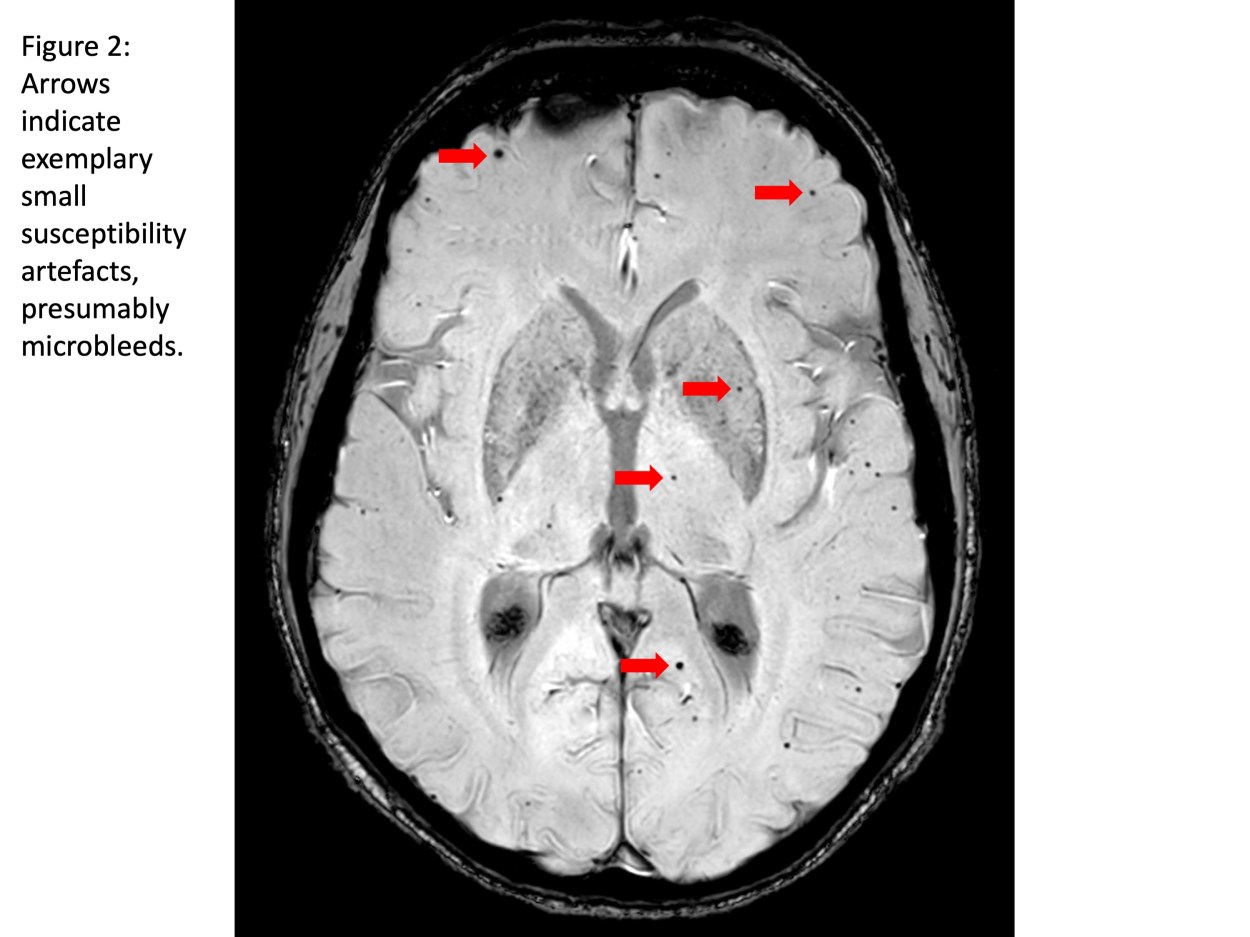
Stroke and cerebral damage are frequent findings after thoracic endovascular aortic repair (TEVAR) with a postoperative clinical stroke rate of 3-4% and silent brain infarcts (SBI) in about 80%.(1-4) However, the mechanism of stroke and subclinical cerebral damage in TEVAR is under-investigated. Current clinical research-efforts such as the STEP-registry (strokes from thoracic endovascular procedures) aim to better understand incidence of, and risk factors for stroke and cerebral damage after TEVAR, and to develop strategies for prevention.(5, 6) More than 60% of patients undergoing arch-TEVAR were reported to have SBIs on diffusion weighted magnetic resonance imaging (DW-MRI) despite protective efforts such as carbon dioxide (CO2) flushing of the endografts.(5, 6) The aim of the current study is to examine the occurrence of CMBs in patients after TEVAR within the STEP-registry and to evaluate their association with patient- and procedural factors.
Ninety-one patients treated with TEVAR in proximal landing zone (PLZ) 0-3 from September 2018 to January 2020 at the German Aortic Center (Hamburg, Germany) and Marie Lannelongue Hospital (Paris, France) were included in the study.(5) The location and number of CMBs were identified and analyzed with regards to procedural aspects, clinical outcome and Fazekas-score as indicator of preexisting vascular leukoencephalopathy.

PelvEx 2024
John T. Jenkins1, Paul Sutton2
1. Consultant Colorectal Surgeon
Chair of Surgery
Lead Complex & Recurrent Cancer Service,
St. Mark's Hospital, London
Imperial College, London
Surgeon to the Royal Household
2. Consultant Colorectal, Pelvic, and Peritoneal Surgeon
Colorectal and Peritoneal Oncology Centre
The Christie NHS Foundation Trust
Chair ACPGBI Advanced Malignancy Subcommittee
DOI: https://doi.org/10.58974/bjss/azbc052
PelvEx 2024 was hosted and organized in London by the ACPGBI Advanced Malignancy Subcommittee and UKPEN. The Royal Institution provided the perfect venue, blending history with excellent facilities which ensured the meeting was a tremendous success. Nearly 300 delegates attended from all over the world, with this year’s meeting having a truly multi-disciplinary programme.
The first day included sessions on “R0 resection – How important is it really”, “How much is too much in exenteration surgery”, and “Mastering morbidity”. In addition, sessions on the “Consequences of exenteration surgery” including patient and nursing experiences, as well as discussion about sex and intimacy, and the psychological consequences of surgery. The day finished with a “Consultants Corner- Grey Heads on Green Shoulders” session discussing a number of diverse challenges encountered at different stages in clinical practice .
The second day began with the inaugural trainee prize presentation session for the now coveted Brunschwig Prize. A number of high quality abstracts were received and the six best (linked below this blog) were invited to deliver oral presentations. The quality was exceptional. This session was followed by sessions on “Research progress” and “Surgical techniques”, followed by an afternoon where the “Oncologists have their say” culminating with a “Global MDT”. The conference was live streamed to China and recorded for posterity.
Thank you to our strategic partners


.png)





Connect