When the first cases of the disease that would have been later named COVID-19 (Coronavirus Disease 2019) caused by SARS-CoV2 were described in Wuhan approximately three months ago, it would have been difficult to predict the impact and the burden that the subsequent outbreak would have had globally. The first case was tracked back to November 2019, indeed the spread COVID-19 proved to be incredibly rapid, and is currently causing several challenges to most health systems.
On the 11th March the World Health Organization (WHO) declared COVID-19 pandemic. Between the last week of February and the first week of March, the number of cases outside China increased 13-fold and the numbers of affected countries tripled. By the time the present piece is being typed, 164 837 cases were recorded globally, with 6470 deaths, 146 countries involved.
Among European countries, Italy has been hit first and more deeply, the reasons for this still being analysed, and no agreed explanation available. Since the first cases were described on the 30th January 2020, two Chinese tourists, the outbreak showed a logarithmic growth, and by today (16/03/2020), the overall number of individuals who tested positive was 24 747 (20 603 still positive) with 1809 deaths. This would mean a mortality rate overall as high as 7.3%, and 43.6% of those who had an outcome. Of those currently infected, approximately 8% is in serious/critical conditions. Lombardy, considered the economic heart of Italy, where an ideal health system is in place, registered the highest number of COVID-19, exceeding 13 200 patients, more than half than all Italian cases. The outbreak is rapidly spreading to the entire peninsula, islands not being spared: almost 1000 cases between South and Islands (3.73%). Even if these figures might not seem worrisome, they actually are, as facilities and infrastructures might not be prepared to afford a similar outbreak as that observed in Northern Italy, and the system could collapse. Restrictive measures had to be taken, and the Italian Government ordered an unpreceded lockdown effective as the 12th March 2020, and its effect and meaning are well testified by the empty Italian cities. Florence’s Uffizi Gallery is closed; St. Peter’s Square in Rome is empty.
These images are self-explanatory. Similar measures are being taken in other European countries, even if the strategies to face COVID-19 were not consistent. Spain followed a similar pathway observed in Italy, with 7753 cases and 288 death as of today, mainly in Madrid, and adopted the same measures.
The impact of COVID-19 on our society is already immense, and some have suggested that the post-pandemic era is likely to blow away the world as we used to know it.
COVID-19 and Cancer
Liang et al. analysed the cases of COVID-19 in China, and found that patients with cancers were at higher risk of developing the symptoms from SARS-CoV2 infection. Out of 1590 COVID-19 cases analysed, an history of cancer was found in 1% of them, versus 0.29% observed in the general population. One out of four had received chemotherapy or surgery within 30 days from infection, whereas another 25% were on follow-up after treatment. This might suggest that cancer patients might be at increased risk, even after curative treatment of the disease, for reasons that are not completely understood. Liang et al. also suggested that severe events were more common in cancer patients with COVID-19, as more patients in this population required invasive treatment measures or died compared with patients without cancer (even [39%] of 18 patients vs 124 [8%] of 1572 patients; Fisher’s exact p=0·0003); the risk was even higher if chemotherapy or surgery were performed in the last month, administered. These findings raise concerns on the ideal care to provide to such patients and whether or not should chemotherapy be continued during the outbreak, or at least stopped or reduced in selected patients at higher risk of infection. Of note, the actual impact of COVID-19 on the outcome of cancer patients in this specific cohort remains to be clearly proven, as the age of this cohort was higher than that of non-cancer patients with COVID-19. Moreover, they were more frequently smokers, and more frequently had polypnea. These considerations advocate for prudence at the time of interpreting the findings of studies which are currently being published on the topic, due to the limited knowledge available and to the relatively low (yet) number of cases described in these publications, which might be underpowered to show clinically relevant findings.
Similar concerns are applicable to patients who are chronically immunodepressed and to those with chronic conditions that might expose them to an increased risk of contracting COVID-19, and with potentially detrimental outcomes.
COVID-19 and usual hospital routine
The effects on COVID-19 on patients with chronic diseases or cancers are more extensive than the risk of contracting the virus for carriers of these conditions. The health system is almost collapsing in several countries, with few available beds in intensive care units. Elective surgery has been stopped in many hospitals, giving priority to cancer patients and to emergency. The personnel is being shortened to the minimum necessary to deliver the basic services, and, while intensive care units and medical wards are saturated, the current appearance of surgical wards is appalling.
Aunque no lo veas, están ahí, trabajando para ti. Sólo tenemos un objetivo: #somostodos, somos #sermas#somosclinicopic.twitter.com/atnSpKCc8x' Julio Mayol (@juliomayol) March 15, 2020
Notwithstanding the effort put in treating as many cancer patients as possible, the timeliness of cures is inevitably delayed, and the outcomes of treatment might well be affected in the long-term. At the same time, screening is not being offered consistently. A delayed diagnosis is associated with worse outcome in cancer surgery. Sanjeevi et al. showed that potentially curable pancreatic cancers had 0% unresectability rate at surgery when the interval between imaging and resection was shorter than 23 days, highlighting the importance of acting within a window of opportunity to achieve optimal survival results. An analysis of a US National Cancer database with over 60 thousands patients with curable colon cancer, found that overall survival was longer in patients operated on within 16 days from diagnosis compared with those operated on after 37 days or more (5-year survival 75.4 vs 71.9%, 10-year survival 56.6 vs 49.7%, both p<0.001). Moreover, the long-term effects and associated indirect costs of cancer surgery include the assessment of lost work-hours due to sick leave after surgery. Postoperative recovery after colorectal cancer surgery might be slower than thought, and advanced disease further impair return to work, suggesting that delaying diagnosis and surgery impacts the economy further.
Free to access in January's BJS: Predicting return to work among patients with colorectal cancer https://t.co/J1oqzrF92k@JJEarnshaw@AmyLightnerMD@bplwijn@des_winter@JohnBeynon5@ksoreide@MalinASund@evanscolorectal@robhinchliffe1pic.twitter.com/9ERKb1C3n7' BJS (@BJSurgery) February 10, 2020
Many chronic conditions are likely to be affected by delayed treatment. Patients waiting for transplantation are another facet to consider. Discussions are ongoing globally in order to face these difficult situations, and how to deal with the current status of things still remains to be clarified.
Patients, family, and COVID-19
During crisis, priorities are being reorganized, meaning that priority is given to patients with more worrisome conditions or those more likely to benefit from a treatment. However, this generates a stressful environment and brings about nonnegligible consequences to individuals’ wellbeing. Surgical patients with conditions that are not being regarded as priority may feel let down by the doctors and the health system, and they need appropriate support to face this new condition, and their families to be cared for, and this will be much more relevant once the current acme of the outbreak has settled. Many societies and patients’ associations have made available for patients’ guidance and suggestions to help them during these difficult times.
Moreover, family visits to patients who are currently being hospitalized are being strictly controlled, so that the postoperative recovery or the in-hospital stay in general are made even more challenging by an overwhelming sense of loneliness.
Facing COVID-19: ongoing initiatives, collaboration
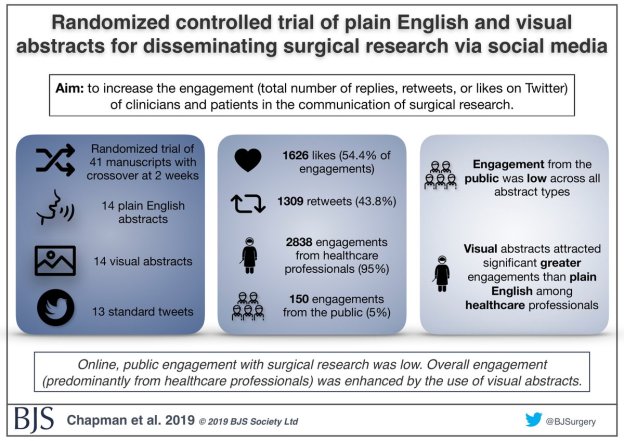
Emergencies can bring to light the worst aspects of humanity, but they can also strengthen the spirit of collaboration against a common issue. Even if many have been forced in isolation or quarantined, even if travel is forbidden from and to several countries, social media proved again to be a powerful means to disseminate knowledge, to facilitate discussions, and to establish collaborative initiatives on a global scale.
The response to the fears of doctors and patients on how to deal with COVID-19 and how to act during the outbreak has been immediate, and several scientific societies have provided documents and platforms to be used as guidance. The Spanish Association of Surgeons (Asociación Española de Cirujanos, AEC) released on the 15th March a Position Statement that can be freely accessed on the measures to be taken for patients needing surgery during the pandemic, and a similar initiative has been announced by the Spanish Association of Coloproctology (Asociación Española de Coloproctología, AECP), with specific focus on patients needing surgery for colorectal conditions. These documents are being developed with an innovative format, meaning that they are solidly grounded on available evidence but they are dynamic, open to updating that can occur within hours.
This is relevant at a time when no agreed policy has been decided to face the COVID-19 pandemic. As of today, not all nations have decided to adopt the same stringent measures acting in Italy and Spain, and likely to be extended to France and other countries. For example, UK has announced a different strategy, relying on the development of an immunity against COVID-19, with no need for restrictive measures. Indeed, this was not agreed by the entire scientific community, and hundreds of UK scientists signed an open letter pressing the Government to enforce social distancing. It is difficult to identify which strategy is the more appropriate, but a common effort towards an agreed strategy is desirable in the following months.
A joint GI Society Message on COVID-19 was released on the 16th March by the American Gastroenterology Association, the American Association for Liver Disease, the American College of Gastroenterology, and the American Society for Gastrointestinal Endoscopy. The document deals with recommendations to provide care, including endoscopy, to patients with gastrointestinal conditions during the pandemic.
The European Crohn’s and Colitis Organisation (ECCO) launched a questionnaire aiming to identify the fears and difficulties that IBD doctors are facing while practising during the COVID-19 pandemic, in order to take actions and provide support. An international, online, secure database has been started to report information on IBD patients diagnosed with COVID-19.
An initiative that rapidly captured the attention of the surgical community globally was the launch of an international prospective registry of patients operated on for whichever condition while positive for COVID-19. The initiative was launched by Aneel Bhangu on the 14th March on Twitter and is open for registration. A draft protocol is available to access and registration can be performed at this link.
#COVID19 and #surgery. Who needs surgery and what are the outcomes? Global study, please join: Any operation, with confirmed COVID or highly suspicious (but no test) at any timepoint.Please register for website access:https://t.co/j3XuGndNXqpic.twitter.com/Xesp9mZxUQ' Aneel Bhangu (@aneelbhangu) March 14, 2020
These initiatives will hopefully help to clarify the actual impact of COVID-19 on surgical patients, and help to define the ideal pathways and perioperative management of these patients.
Impact on psychical well-being of healthcare professionals: who cares for the carers?
Last but not least, healthcare professionals are being exposed on the frontline. They are working in extremely difficult conditions, far different from what most of them were trained to work. The intensely stressful conditions in which doctors, surgeons and all healthcare professionals are called to work, is exposing them and their families to unpredictable consequences.
Not being able to treat everyone, the need to do extra shifts, wearing protective equipment during the entire shifts as well as the lack of protective devices, the fear of getting infected, all contribute to a potential burnout.
Doctors are choosing to isolate themselves from their relatives, in order to protect them, even if asymptomatic. The fear of being tested positive, apart from the fact that being affected already implies, brings about the necessity of being quarantined, and further reduces the number of available team members. This is further aggravated by the required quarantine for those colleagues who were in contact with the index healthcare professional tested positive.
Indeed, many institutions and entities are providing help to doctors struggling with the current crisis. The Physician Council of Barcelona (Colegio de Medicos de Barcelona, COMB), for example, established a telephone-based service to support doctors who are experiencing psychological stress and difficulties while in isolation, and a similar service was offered to struggling doctors at local hospitals (e.g. Hospital Vall d’Hebron in Barcelona). Similar initiatives are needed, and must not be limited to the emergency only, but should last long after this has been controlled.
Things are changing rapidly with COVID-19. A financial crisis is likely to occur, that will require to be faced jointly when the emergency has been resolved. It is however needed to maintain our focus on what we are doing every day with every single patient, and those of us who are isolated need not to forget that this is part of caring for the others. Doctors, surgeons, nurses, all the healthcare professionals need to feel backed by the institutions and by the people. In Italy and Spain, people under lockdown have started clapping their hands as a tribute to healthcare professionals. During such difficult times, similar spontaneous acts are fuel for our practice and help us to cope with the burden and the negativity that COVID-19 has spread, while scanning the horizon in search of the end of the current crisis.
A normal Saturday night during #COVID19 in #BarcelonaAlmost desert streets; people in their houses applaud doctors and health workers…breathtaking 😊thank you!!#YoMeQuedoEnCasa#iorestoacasa#andratuttobene#TodoIraBien#lovespain#SoMe4Surgery#staysafe❤💛❤ pic.twitter.com/H2GcjYXcdv' Gianluca Pellino (@GianlucaPellino) March 14, 2020




.png)




