It is becoming increasingly common to dedicate days, or even months, to ‘health awareness’. These events should help people to learn about these conditions. From these, we can hope that people might learn about symptoms that help them get a diagnosis, or learn about new treatment options for their conditions. It also provides a focal point where we can come together as a community to recognise those impacted, and find ways to address these serious health conditions. It may even act as a clarion call, moving charities, governments, and individuals, to make efforts to fund and deliver research to further understand and improve outcomes for these conditions.
The BJS Academy, alongside BJS & BJS Open, feel it is an important part of our mission to contribute to these awareness months. So much research is published with enthusiasm, but then resides solely within the pages of a journal (or latterly, as a lonely PDF on a server). It is important to ensure that new information is shared with people who might find it useful. This is particularly important when it comes to conditions which currently have a poor prognosis, or may affect only a small number of people. With this in mind, our team will contribute to the online discussion for disease months by highlighting 2-3 papers from BJS and BJS Open, and sharing them across our social media channels. This will include a short summary and a link to the paper.
This move comes as part of our commitment to sharing key clinical research to support the knowledge of surgeons around the world, and to ensure our patients receive care informed by evidence of the highest possible standard.
February is Oesophageal Cancer awareness month. So many people around the world will have been affected by this as patients, family and friends. Many challenges exist in the treatment of oesophageal cancer. First, issues around late diagnosis. In this context, disease may be locally advanced with a large tumour that is difficult to remove surgically, with lymph nodes present, or with metastatic disease. How can we best identify people at early stages of this condition? Where people present with locally advanced disease, what is the best strategy to achieve local and systemic control? Importantly, how do we support patients psychologically and nutritionally around this time? These are important questions, particularly for surgeons, and affected patients before we think about surgery, adjuvant therapy, follow-up, and long term effects of treatment. Our colleagues Drs Tejedor and Schneider have selected papers published in our journals over the last year that they believe contribute to wider discussions around this condition. We present this for your consideration and discussion, as we work to improve outcomes from this common cancer.
______
BJS highlights:
______
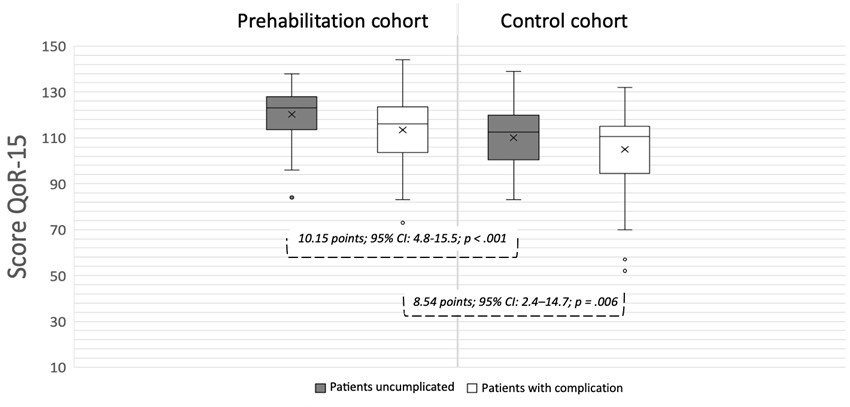
Association of Upper Gastrointestinal Surgery of Great Britain and Ireland (AUGIS)/perioperative quality initiative (POQI) consensus statement on prehabilitation in oesophagogastric surgery
This study used a modified Delphi process through POQI conferences to gain consensus on 20 statements regarding prehabilitation in oesophagogastric cancer (OGC) patients undergoing surgery. Multidisciplinary experts agreed that multimodal prehabilitation, incorporating exercise, nutrition, and psychological support, should be considered standard care. Key outcomes such as improved postoperative recovery and reduced complications were strongly supported, although some areas, like length of stay and chemotherapy response, had weaker evidence. The study also highlighted significant barriers, including funding and manpower, and identified the need for future research to refine prehabilitation interventions. Read the paper.
______
Pathological response to neoadjuvant chemoradiotherapy for oesophageal squamous cell carcinoma in Eastern versus Western countries: meta-analysis
This meta-analysis compared pathological complete response (pCR) rates to neoadjuvant chemoradiotherapy in oesophageal squamous cell carcinoma (OSCC) between Eastern and Western countries. A systematic review and multi-level meta-analysis of 51 Eastern (5636 patients) and 20 Western cohorts (3039 patients) found lower pCR rates in the East (31.7%) than in the West (40.4%) (P = 0.003). The observed disparity could not be fully explained by patient, tumour, or treatment differences, suggesting potential genetic or environmental influences. Read the paper.
______
Laparoscopic or open abdominal surgery with thoracotomy for patients with oesophageal cancer: ROMIO randomized clinical trial
The ROMIO study is a RCT involving 547 participants, with 276 in the hybrid surgery group and 271 in the open surgery group. The primary outcome, patient-reported physical function, showed no significant difference between the groups at 30 days post-surgery. The risk of major complications was slightly lower in the open surgery group (57%) compared to the hybrid surgery group (64%). Additionally, the 95% confidence interval for the treatment effect on physical function did not include the minimum clinically important difference of 10.4 points, indicating no meaningful difference between the two surgery groups. While hybrid surgery had slightly higher procedure costs, these were not compensated by lower subsequent inpatient or outpatient care costs. Read the paper.
______
Recurrence-free survival as a surrogate endpoint for overall survival after neoadjuvant chemotherapy and surgery for oesophageal squamous cell carcinoma
This retrospective, multicenter observational study evaluated recurrence-free survival (RFS) as a surrogate endpoint for overall survival (OS) in patients with esophageal squamous cell carcinoma (OSCC) undergoing surgery after neoadjuvant chemotherapy. Using individual patient data from 3,154 participants across 58 Japanese hospitals, the study used the illness–death model to uncover a strong connection between RFS and OS (Kendall's τ = 0.797). Subgroup analyses revealed that the correlation was stronger in patients with better pathological responses, and exploratory analyses showed limited correlation between pathological complete response (pCR) or pathological grade and OS. Read it here.
______
BJS Open highlights:
______
Surgical and multimodal treatment of metastatic oesophageal cancer: retrospective cohort study
This retrospective study analyzed survival outcomes in patients with oligometastatic esophageal cancer treated with different modalities, including surgery, multimodal therapy, chemotherapy alone, and best supportive care. Patients undergoing surgical resection or multimodal therapy with surgery demonstrated significantly improved survival (median 19.0 and 18.0 months, respectively) compared to chemotherapy alone (11.0 months). These findings suggest that selected patients with oligometastatic disease may benefit from surgical interventions. Read the paper.
______
Robot-assisted minimally invasive oesophagectomy versus thoracoscopic approach: multi-institutional study on short-term outcomes
This multi-institutional study compared short-term outcomes of robot-assisted minimally invasive esophagectomy (RAMIO) and conventional minimally invasive esophagectomy for esophageal squamous cell carcinoma. RAMIO was associated with superior outcomes, including higher lymph node retrieval (especially at the level of the laryngeal nerve), reduced pneumonia rates, and shorter hospital stays, especially in patients with high comorbidity or receiving neoadjuvant therapy. The results underscore the potential of robotic techniques in enhancing intraoperative precision and postoperative recovery. Read the paper.
______
Sex-related differences in oncologic outcomes, operative complications and health-related quality of life after curative-intent oesophageal cancer treatment: multicentre retrospective analysis
A multicenter analysis revealed sex-based disparities in oncologic and quality-of-life outcomes following curative treatment for esophageal cancer. Female patients had better overall and disease-free survival, particularly in adenocarcinoma, but experienced higher rates of major postoperative complications. Males reported better physical functioning and overall quality of life but had more financial concerns. These findings highlight the need for tailored care strategies to optimize outcomes across sexes. Read the paper.




.png)



