As Monty Python would say…
Time for an upbeat blog!
The BJS ‘how to write a paper’ session is a fixture at many UK surgical meetings. This covers lots of the ‘nuts and bolts’ of writing a paper. We delivered a short version of this course at the Association of Surgeons in Training Meeting in Birmingham.
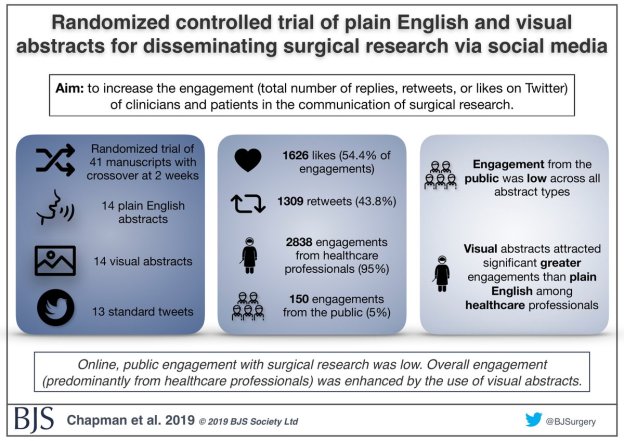
One of the fun and developing parts of publishing is the promotion of material on social media. Visual abstracts have emerged as a concise way of sharing the key points of a manuscript online. Therefore it shouldn’t come as a surprise that we cover making visual abstracts in this course.
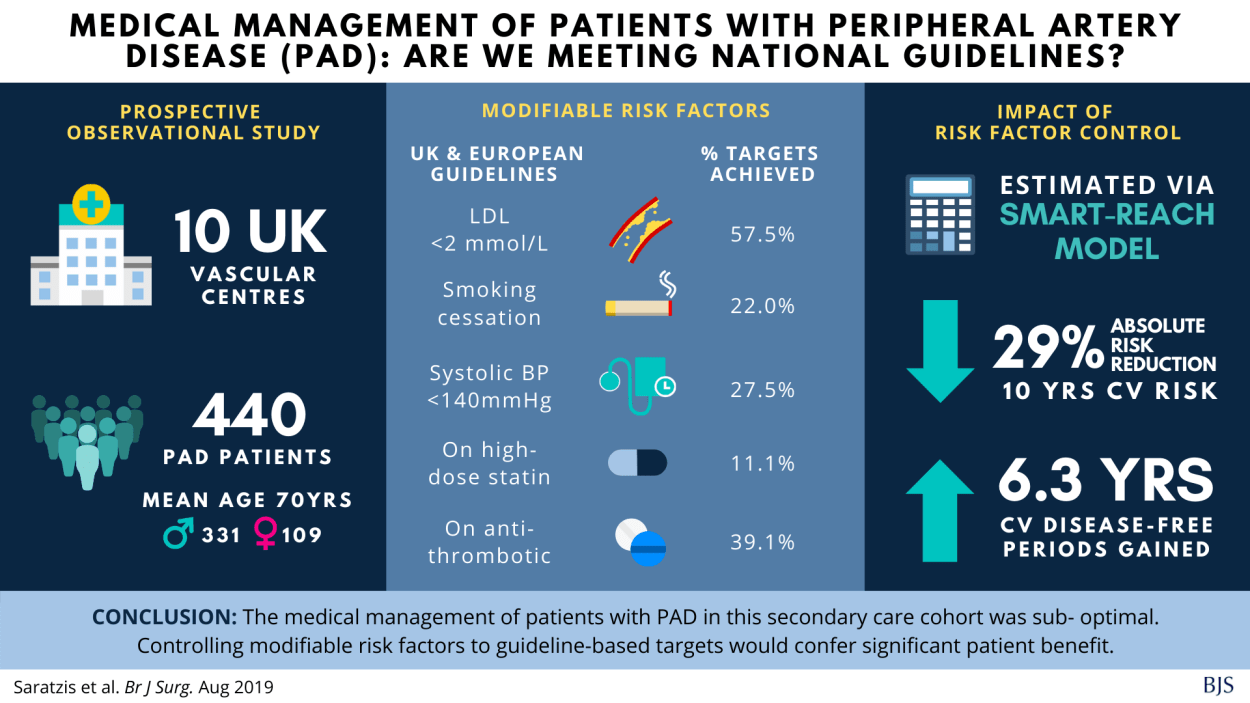
We discuss things like picking out key points and the use of icons and images. We then give the participants a choice of two abstracts and invite them to submit a visual abstract to our competition. This year we chose this paper on peripheral vascular disease and this paper on oesophageal cancer as subjects for the exercise.
We were pleased to receive a number of visual abstracts, which were of a really high standard. Most participants opted for the peripheral artery disease abstract. The team were really impressed by the abstracts that were submitted to us. Dr Jia Ying Lim (blue background) was the winner, and Dr Rucira Ooi (red background) was awarded the runner up prize. You can see these below.
Please keep an eye out for the course at future meetings. If you would like us to deliver this course at your meetings, please get in touch!



.png)




