Eight surgeons came together to review the available evidence on the management of rectus diastasis and produce evidence-based guidelines. Sadly the evidence quality ranged from very low to moderate. Despite this, the team were able to provide nine recommendations, with the strength of the recommendation ranging from weak to strong.
The nine key questions were:
KQ1 What is the definition of RD?
KQ2 Which modalities are most suitable for diagnosis and assessment of RD?
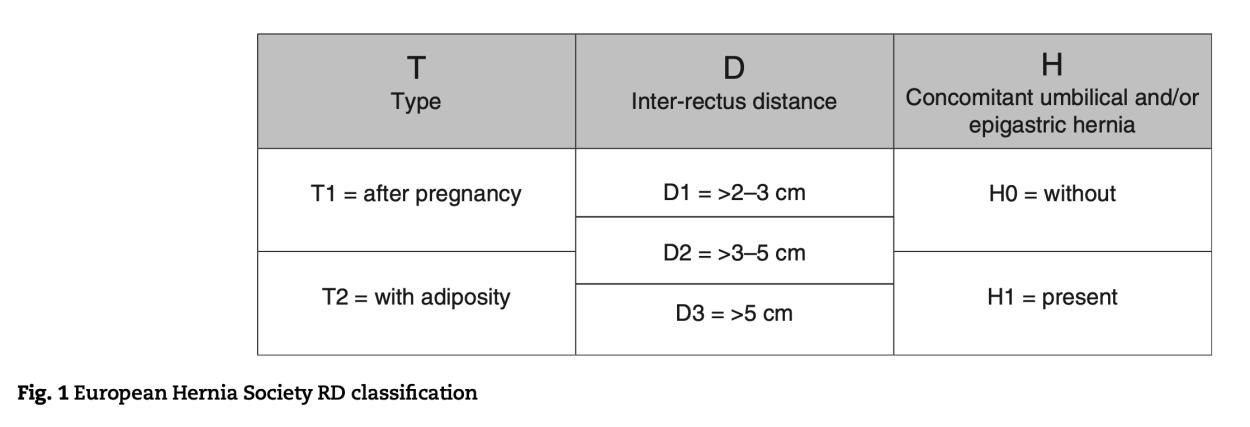
KQ3 What are the classification systems for RD?
KQ4 What symptoms are associated with RD?
KQ5 Which outcome measures should be used to evaluate treatment for RD?
KQ6 Are there non-operative treatment options for RD?
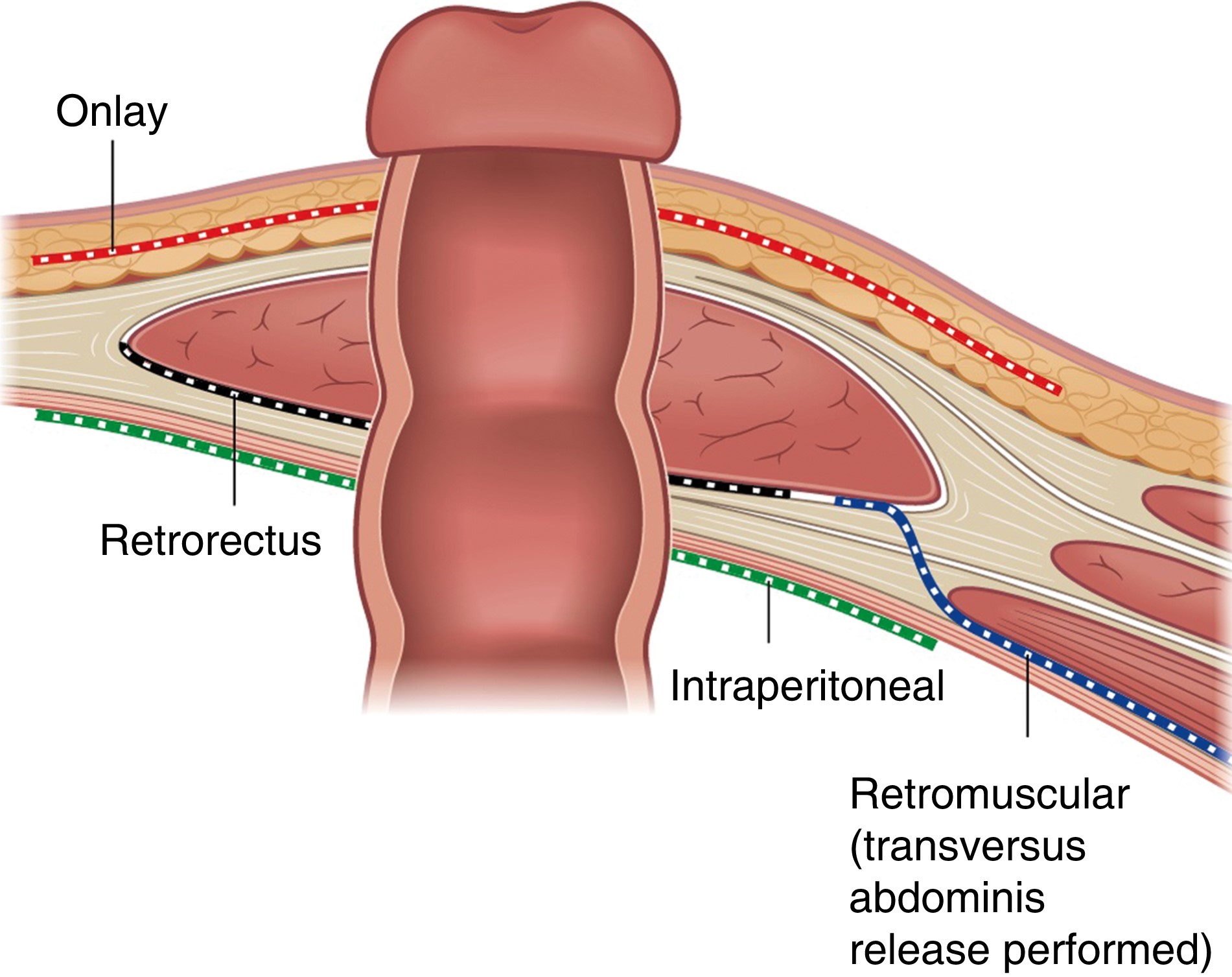
KQ7 What are the surgical treatment options in patients without concomitant hernias?
KQ8 What is the optimal treatment of rectus diastasis with concomitant umbilical or epigastric hernias?
KQ9 Is there a role for specific postoperative management of RD repair?
This is clearly an area of surgery where higher-quality research is needed; until that is achieved, these guidelines, together with detailed, honest, and open discussions with patients, offer the best pathway towards shared, evidence-based, decision making.



.png)




