From idea to practice.
The transperitoneal (TP) approach to colorectal surgery (both laparoscopic and robotic) has never made sense to me even after many years of performing both techniques. From a colorectal perspective, every important anatomical structure is a retroperitoneal structure. The peritoneum itself is an under-appreciated, under-utilised organ. When trespassing in the peritoneal cavity, the small bowel and omentum present significant unnecessary challenges especially in the obese and those with previous surgery. The whole experience could sometimes feel like trying a knife and a fork for the first time.
Multiport wristed robotic instruments have just made an awkward laparoscopic TP procedure less so. There is a design fault with TP access. There is no doubt, however, that the TP access works in many straightforward operations and this piece is not in any way a call to abandon TP access. However, some 10-25% of operations are responsible for 75-90% of a challenging, long, and painful operation (for patient, surgeon, assistant, and anaesthetist).
I wondered whether an extraperitoneal (XP) approach in colorectal surgery could help improve further on the drawbacks of TP surgery. I gained my experience in the XP space while performing TEP hernia repair.
The first challenge was to find and test the concept on cadavers. This has taken a long time, but we were fortunate enough to get initial support from Intuitive Surgical to use their Xi robot to perform XP dissections in cadavers. We received further support from Lancashire Teaching Hospitals’ Trustee Bursary Award to develop our own dissections using laparoscopic instruments during 2018 and 2019. In my opinion, the most important aspect of an innovation is to have a supportive team, governance structure and medical leadership without, which it is almost impossible for any innovation to develop.We were not successful using the multiport robot in the narrow XP space. The first team that I gathered considered this a failure and their support stopped at this stage. Pivoting to standard laparoscopic instruments and getting further support from my current team and co-authors have taken the technique further and we were able to perform a whole low anterior resection procedure using the XP approach in cadavers using standard laparoscopic instruments.
A specific challenge came up when the local ethics committee asked for an external opinion on the technique (figure 1) This was a long and frustrating journey as I was essentially asking (in vain) those who never heard of the concept for validation.
The journey was not easy but having a clear vision, personal characteristics (passion, acting. resilience) and the right relationships have all helped navigate many challenges. We are all naturally sceptical about change and high standards of safety need to be achieved before we could start to appreciate positive change.
We have so far completed some 70 live procedures. We have published and presented data on cadaveric and clinical experience including the latest original article in the BJS. We continue to develop the technique to achieve its maximum potential. We look forward to discussion about the concept and its possibilities.
https://sketchfab.com/3d-models/expert-surgery-3d-animation-e9d8305360c845899a318a1c52cf349fFig (2) 3D animation of XP versus TP approach- the model could be rotated.
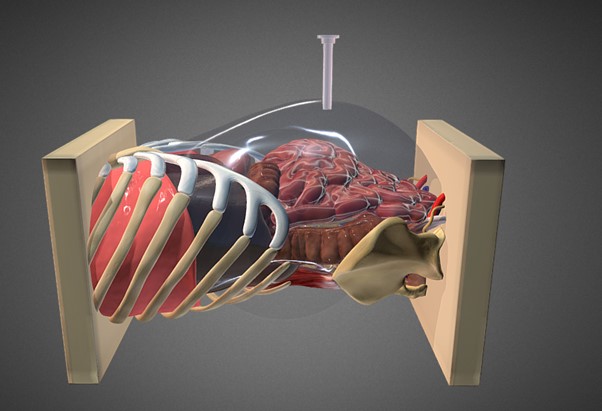



.png)




